by Clear Path Intervention
Share
by Clear Path Intervention
Share
")
In most of the country, the question facing a family is whether a loved one will accept treatment. In Alaska, there is a second question stacked on top of the first. If they say yes, where exactly do they go, and how do they get there before the willingness fades?
That second question is not a logistical footnote. It is one of the defining features of addiction in the largest, least densely populated state in the union, and it shapes everything from overdose risk to the odds of staying in care. The 2026 data tells a story of fragile, uneven progress laid over a geography that makes recovery uniquely hard to reach.
A small decline against a very steep climb
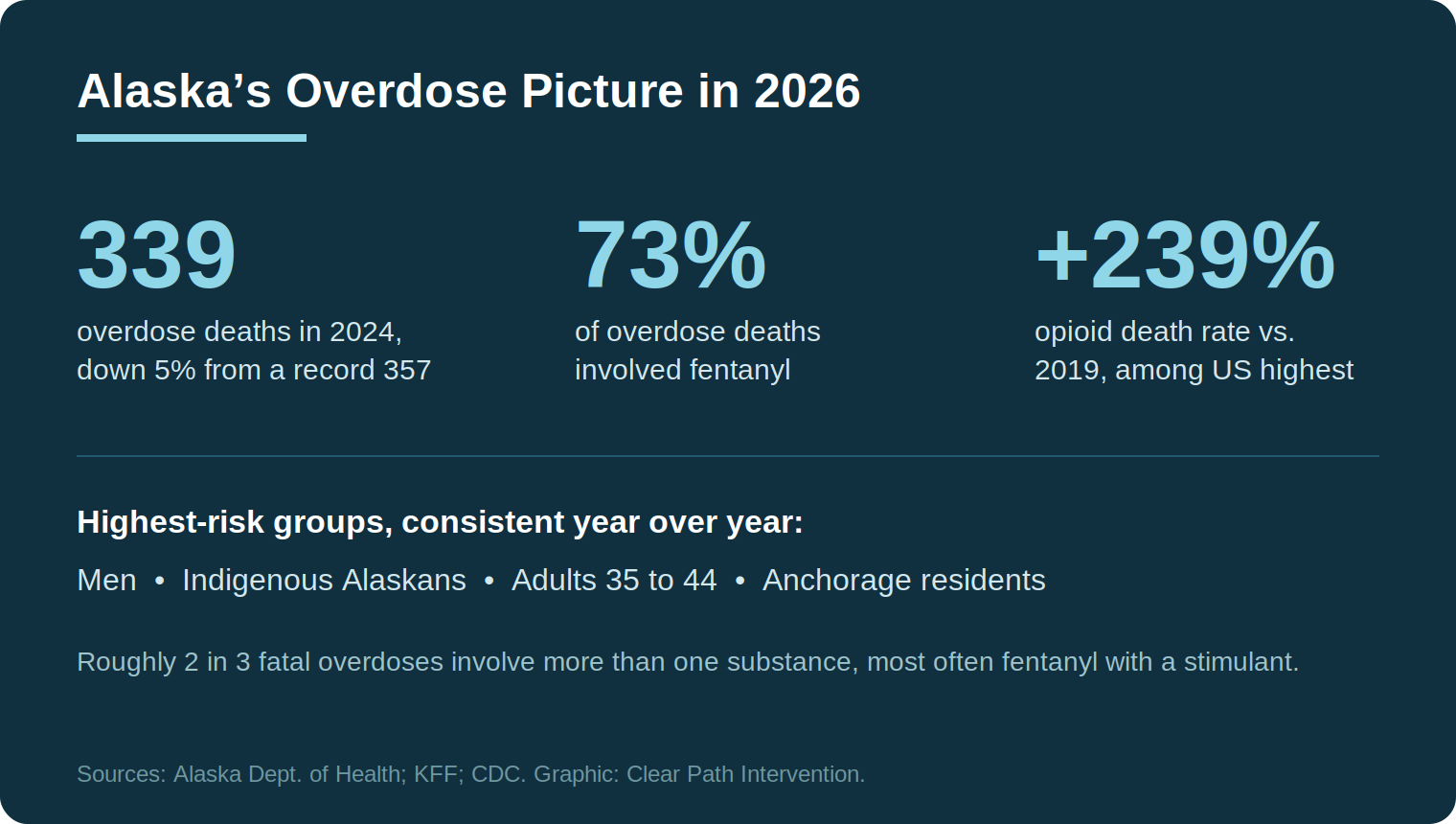
The encouraging figure first. According to an annual report from the Alaska Department of Health, 339 people died of drug overdoses in Alaska in 2024, a five percent decline from the record high of 357 the year before. State officials credited a portion of that improvement to the distribution of tens of thousands of naloxone kits, expanded medication-assisted treatment, recovery housing, and mobile crisis teams now operating in Anchorage, the Mat-Su, Fairbanks, Ketchikan, and Juneau.
Now the sobering context. Alaska’s decline was far smaller than the national one, and it follows a climb that stands out even in a country full of bad numbers. A KFF analysis of state-by-state opioid trends found that Alaska had one of the largest increases in opioid overdose death rates in the nation relative to 2019, on the order of more than two hundred percent. A modest one-year dip does not undo a multi-year surge of that magnitude. It interrupts it, at best.
Fentanyl drives the crisis here as it does nearly everywhere, contributing to roughly three quarters of the state’s overdose deaths. But the Alaska data underscores a pattern that national reporting often glosses over. Most fatal overdoses in the state involve more than one substance, frequently fentanyl combined with a stimulant such as methamphetamine. The single-drug overdose has become the exception. That polysubstance reality changes the clinical picture and, as discussed below, changes what effective help has to account for.
Who the data points to, and why it matters
State health officials note that the Alaskans at highest risk have stayed remarkably consistent over recent years: men, Indigenous Alaskans, residents of Anchorage, and adults between 35 and 44. National data echoes the disparity affecting Native communities. NIDA and CDC analyses have repeatedly found that American Indian and Alaska Native populations experience among the highest rates of fentanyl-involved overdose, a disparity rooted in a tangle of factors including historical trauma, geographic isolation, and uneven access to culturally grounded care.
That last point deserves emphasis, because it is easy to read a list of risk groups as a list of stereotypes. It is the opposite. These patterns reflect where the system has failed to reach people, not anything inherent about the people themselves. A family in a remote community is not at higher risk because of who they are. They are at higher risk because the nearest detox bed might be a plane ride away.
Distance as a clinical problem
This is where Alaska genuinely differs from the rest of the country. In most states, the gap between deciding to get help and arriving at treatment is measured in hours. In much of Alaska, it is measured in flights, weather windows, and the simple fact that many communities are not connected to the road system at all. Juneau, the state capital, cannot be reached by car. Neither can large stretches of the state.
Why does that matter clinically? Because the willingness to enter treatment is often a narrow window rather than a settled decision. The brain changes that NIDA documents in its research on the science of addiction include disruptions to motivation and decision-making, which is part of why a loved one can mean a yes today and reverse it tomorrow. When the yes has to survive a multi-day journey to a distant facility, the geography itself becomes a risk factor. Every hour of delay is an hour for ambivalence to return.
Alcohol, the quieter Alaskan epidemic
Fentanyl dominates the overdose conversation, for good reason. But any honest account of substance use in Alaska has to reckon with alcohol, which causes harm on a scale that rivals the drug crisis while drawing a fraction of the attention. The state has long carried one of the highest rates of alcohol-related death in the country, claiming hundreds of lives a year. That toll is woven into the same conditions that shape the overdose numbers: isolation, long and dark winters, thin access to care, and, in some communities, the intergenerational weight of historical trauma.
For families, the implication is direct. The substance threatening a loved one in Alaska is at least as likely to be alcohol as an illicit drug, and the two often travel together. Alcohol use disorder is no less a medical condition than opioid use disorder, and the CDC’s data on excessive alcohol use places it among the leading preventable causes of death in the country. It responds to the same fundamentals as any other substance disorder: accurate assessment, a structured plan, and timely entry into care. The reason to name it here is that families sometimes treat a drinking problem as less urgent than a drug problem. In Alaska, the numbers do not support that hierarchy.
How the crisis looks across Alaska’s communities
The interventionists who work with families across Alaska encounter very different versions of the same underlying problem depending on where a family lives.
Anchorage
Home to a large share of the state’s population, the Anchorage area carries the state’s highest overdose rate and also the deepest concentration of its treatment resources. For families in the city, care is comparatively close. The challenge is the same urban-supply intensity seen in larger Lower 48 metros, where availability accelerates the progression of a developing addiction.
Fairbanks and the Interior
Further north, families in the Fairbanks region contend with extreme seasonal isolation and long, dark winters that are independently associated with heavier alcohol and stimulant use. Resources thin out quickly outside the city, and the distances families must cover to reach specialized care grow accordingly.
Juneau and Southeast Alaska
In Juneau and the Southeast, the absence of road access turns every treatment decision into a travel decision. This is the part of the country where the logistics of getting a willing person to a treatment bed, safely and without losing momentum, can matter as much as the clinical plan itself. Coordinated transport, sometimes to facilities outside the state, becomes a central rather than peripheral concern, and is one reason sober transport features so heavily in Alaskan cases.
What effective help has to account for in Alaska
Pulling these threads together points to a few principles that the evidence and the geography both support.
First, the plan has to be built before the conversation, not after. Family-based approaches with the strongest research support, including the CRAFT model documented in the clinical literature gathered by SAMHSA, share an emphasis on preparation and on coaching the family rather than confronting the individual. In Alaska, preparation also means having a treatment placement and a route to it identified in advance, so that a yes can be honored immediately.
Second, polysubstance use should be assumed, not discovered. Because most fatal overdoses in the state involve a mix of drugs, a plan built around a single substance often misjudges the clinical reality. Honest assessment of what a person is actually using is a first step, not a formality.
Third, momentum is the scarce resource. The further a family is from services, the more the success of any plan depends on compressing the time between decision and admission. That is a practical insight rather than a clinical one, but in a state this large, the practical and the clinical are inseparable.
It is worth ending the practical points on a development that cuts the other way. Alaska has expanded telehealth-delivered counseling and medication for opioid use disorder, which together begin to close some of the distance that has long defined care in the state. A person in a remote community can, in a growing number of cases, begin medication and therapy without first traveling hundreds of miles. None of that removes the need for in-person care, or for the structured family planning described above, but it does mean the geographic obstacles, while still formidable, are not quite as absolute as they once were.
The 2026 picture, then, is genuinely two-sided. Alaska is doing some things that work, and the death count has responded. At the same time, the state remains among the hardest places in the country to be a family trying to move a loved one from danger into care, not because the people are different, but because the map is. Understanding that distance is itself a risk factor is the starting point for thinking clearly about what to do.
National and state context is maintained by the CDC overdose prevention center and KFF’s state health data. Anyone in immediate crisis can reach the SAMHSA National Helpline at 1-800-662-HELP or dial 988. In Alaska, the statewide Careline can be reached at 988 as well.
HELP IS AVAILABLE
Do You Have a Loved One Struggling with Addiction or Mental Health Issues?

California does not fit the story most people carry in their heads about the overdose crisis. It is, by prescribing measures, one of the most cautious states in the country. It also contains some of the most visible, concentrated drug crises in America. Both things are true at once, and holding them together is the […]

Every state’s addiction story has a starting point. In Arkansas, more than in almost anywhere else in the country, that story began at the pharmacy counter. For years the state has led or nearly led the nation in how many opioid prescriptions its doctors write, and that history still shapes the crisis families face today. […]

The national story about overdose in 2026 is, for once, a hopeful one. Deaths have fallen for several years running. Arizona is the exception to that story. While the rest of the country has been recording its first sustained relief from the fentanyl crisis, Arizona has been moving in the opposite direction, and the gap […]

For the first time in nearly a decade, Alabama is recording fewer overdose deaths than it did the year before. That is worth saying plainly, because families living inside the addiction crisis rarely hear good news. In January 2026, state outlets reported that more than 900 Alabamians died of drug overdoses in the most recent twelve-month […]