by Clear Path Intervention
Share
by Clear Path Intervention
Share

Every state’s addiction story has a starting point. In Arkansas, more than in almost anywhere else in the country, that story began at the pharmacy counter. For years the state has led or nearly led the nation in how many opioid prescriptions its doctors write, and that history still shapes the crisis families face today. Understanding the connection is not about assigning blame. It is about seeing clearly how a person ends up dependent, so the path back into care makes sense.
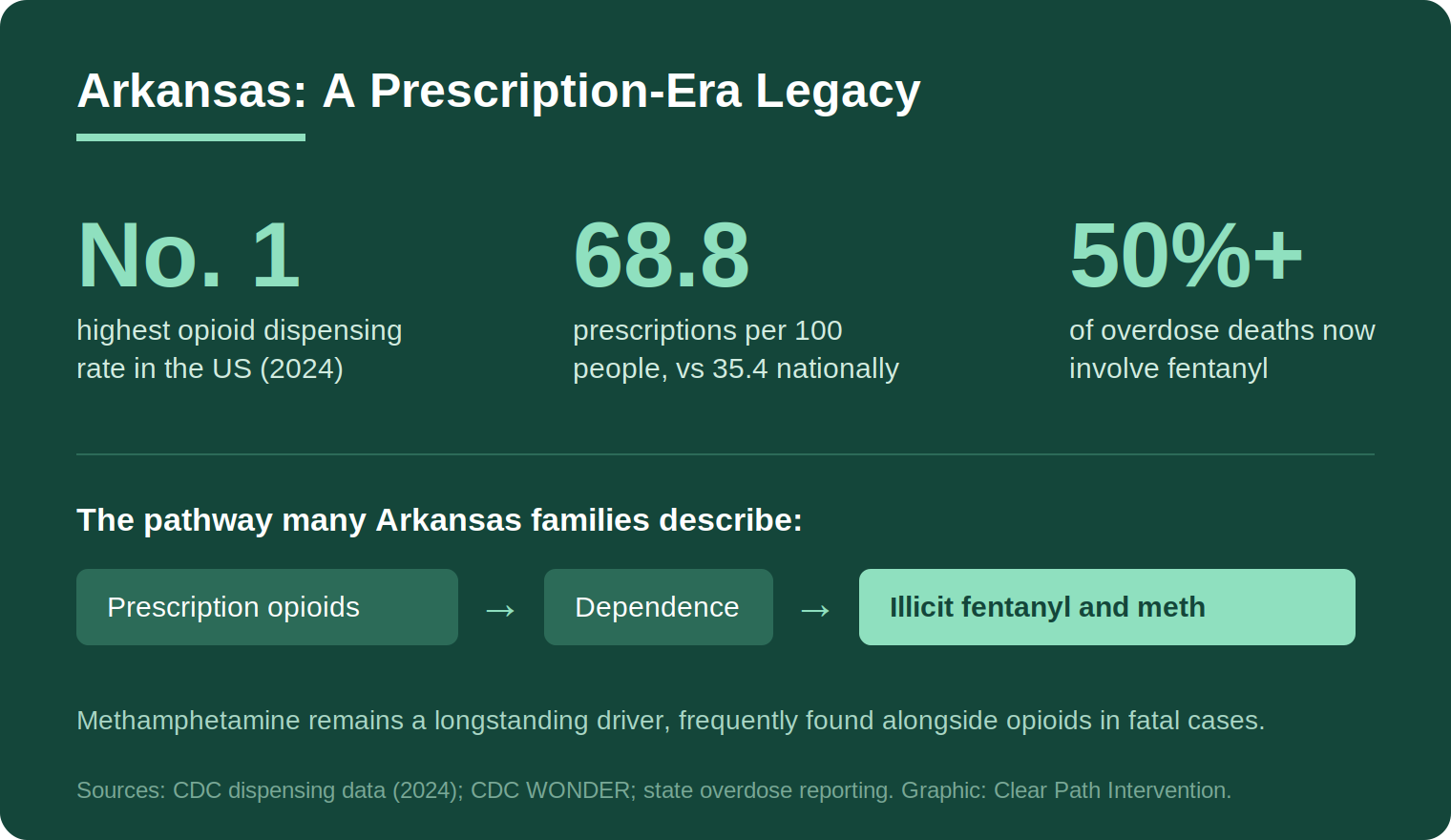
The most recent federal data makes the pattern hard to miss. According to the CDC, in 2024 Arkansas had the highest opioid dispensing rate of any state, at 68.8 prescriptions per 100 people, nearly double the national rate of 35.4. That is not a relic of the past. It is current. And it sits underneath a drug supply that has since turned far more lethal than any prescription pad.
How a prescribing pattern becomes an addiction problem
It helps to be precise about cause and effect here, because the link between prescriptions and addiction is often described too loosely. The vast majority of people who take an opioid for legitimate pain do not develop a substance use disorder. But when prescribing is widespread and sustained across an entire population, the math changes. A higher volume of prescriptions means more leftover pills in medicine cabinets, more opportunities for early exposure, and more people who develop physical dependence and then find themselves cut off when a prescription ends.
That last moment is the dangerous one. A person who has become dependent, then loses access to a legal supply, does not simply stop. The body has adapted. The National Institute on Drug Abuse explains that repeated opioid exposure produces real changes in the brain regions governing judgment, reward, and self-control, changes documented across its research on drug misuse and addiction. Those changes are why willpower alone so rarely resolves the problem, and why the transition from prescription pills to whatever is available on the street can happen faster than a family expects.
The supply that waited at the end of the pipeline
What is available on the street today is not what it was a decade ago. Illicitly manufactured fentanyl has saturated the drug supply nationwide, and Arkansas is no exception. State and regional reporting indicates that fentanyl is now involved in more than half of the state’s overdose deaths. Methamphetamine, which never left Arkansas the way it faded in some regions, remains a major driver and increasingly turns up alongside fentanyl in the same fatal cases.
This polysubstance reality matters for families trying to understand what they are dealing with. A loved one who began with prescribed pain medication may now be using something entirely different, often without knowing exactly what is in it. The national picture, tracked by the NIDA overdose statistics, shows fentanyl and stimulants increasingly combined, which complicates both the medical risk and the treatment plan. The pathway that started with a prescription rarely stays there.
Why the prescribing history still matters for Arkansas families
There is a practical reason to understand this history rather than treat it as background. Families in Arkansas are more likely than families in most states to be dealing with an addiction that began with a legitimate medical event: surgery, a back injury, chronic pain. That origin shapes how the person sees themselves. Someone who never intended to use drugs, who started with a doctor’s prescription, often resists the label of addiction precisely because it does not match their self-image. They were following medical advice. How could this be that.
That resistance is understandable, and it is also one of the reasons direct confrontation tends to backfire. The more useful frame, and the one supported by the science, is medical. Substance use disorder is a treatable chronic condition, not a moral failing or a character flaw. Meeting a loved one with that understanding, rather than with judgment, tends to lower the defensiveness that keeps people out of care.
How the crisis looks across Arkansas
Arkansas is a largely rural state, and that geography shapes both the problem and the available help. The interventionists who work with families across Arkansas encounter very different circumstances depending on where a family lives.
Little Rock
The state’s capital and largest metro holds the deepest concentration of treatment resources in Arkansas, which gives families in the Little Rock area a relative advantage in reaching care. The central-Arkansas fentanyl supply mirrors the national pattern, and the proximity of services means the gap between a decision and an admission can be short, if a family is prepared to act.
Northwest Arkansas
The fast-growing Fayetteville and Springdale corridor has drawn a young, mobile workforce, and with it the pressures that accompany rapid growth and a large student population around the University of Arkansas. Addiction here often hides behind professional and academic success, which can delay the point at which a family treats the situation as urgent.
Fort Smith and the river valley
Closer to the Oklahoma border, the Fort Smith region contends with the rural-access problem that defines much of the state. Specialized treatment can be a significant drive away, which makes preparation and logistics a real part of any plan rather than an afterthought.
Treatment options, and the stigma that delays them
One reason families in prescription-heavy states hesitate is confusion about what treatment actually involves. For opioid use disorder specifically, the strongest evidence supports medication-assisted treatment: medications such as buprenorphine, methadone, or naltrexone used alongside counseling. These medications are not, as an older stigma held, simply substituting one drug for another. They are the medical standard of care, and research consistently shows they reduce the risk of fatal overdose and help people stay in recovery far more reliably than willpower alone. A family weighing options for a loved one should know that medication-based treatment is evidence-based, not a compromise or a sign of weakness.
Stigma is its own obstacle, and it tends to weigh heaviest in smaller communities where everyone knows everyone. A person who began with a legitimate prescription may feel a particular shame at being told they have an addiction, and a family may share the instinct to keep the problem quiet. That secrecy, understandable as it is, often delays care. Treating the condition as the medical problem it is, rather than a private failing to be hidden, is frequently the first practical step toward getting help. Co-occurring conditions such as depression, anxiety, or chronic pain are common and treatable, and a good assessment looks for them rather than treating the substance use in isolation.
What the evidence says about getting someone into care
Because the word intervention carries a dramatic, televised connotation, it helps to separate the spectacle from the practice. There is no single technique called intervention. There are several structured approaches, and the credible ones share an emphasis on preparation rather than ambush.
The Johnson Model, the version most people picture, gathers a prepared group to express concern and present a clear request to enter treatment. Family-systems approaches such as ARISE, and the research-supported CRAFT method (Community Reinforcement and Family Training), take a more gradual, less confrontational path and put significant weight on coaching the family rather than confronting the individual. CRAFT in particular has a notable evidence base, with controlled studies finding that training family members in specific communication and reinforcement strategies brings a substantial share of previously resistant people into treatment. The clinical guidance compiled by SAMHSA consistently points the same way: structured family involvement improves outcomes.
In a rural state, one element deserves extra attention. The plan should include a treatment placement and a route to it arranged in advance, so that a yes can be acted on the same day rather than lost during a long delay. Momentum matters everywhere. It matters more when the nearest appropriate facility is two hours away. Honest assessment of what a person is actually using, given the polysubstance pattern, is also a first step rather than a formality.
None of this requires a family to have everything figured out before they begin. It requires accurate information and a willingness to approach the problem as the medical condition it is. Arkansas did not arrive at its current situation by accident, and no single family caused their loved one’s addiction. Seeing the pathway clearly, from the prescription counter to today’s supply, is what allows a family to respond to where their loved one actually is, rather than where the story started.
It is also worth saying plainly that families do not have to wait until they are sure of every detail. The interventionists who work in rural states routinely help families who know only that something is wrong and that their own efforts have stopped working. That is enough to begin. Clarity about the diagnosis and the plan tends to come through the process rather than before it.
For continuing context, the CDC overdose prevention center and NIDA both publish regularly updated national and state data. Anyone in immediate crisis can reach the SAMHSA National Helpline at 1-800-662-HELP or dial 988.
HELP IS AVAILABLE
Do You Have a Loved One Struggling with Addiction or Mental Health Issues?

There is a particular kind of exhaustion that comes from loving someone whose drug addiction has taken over their life. You have had the conversations. You have made the threats — and not followed through. You have set boundaries — and let them slip. You have searched online at 2 a.m. and closed the laptop […]

When a family is in crisis — when a loved one’s addiction has reached the point where something has to happen — the pressure to act quickly can make it hard to think clearly about who to call. The intervention field is largely unregulated. Anyone can call themselves an interventionist. The quality of services ranges […]

Families who are new to this process often have a narrow picture of what a professional intervention service involves. A specialist shows up, talks to the family for a bit, sits in the room during the conversation, and leaves. That picture is missing most of what actually happens — and most of what makes the […]

Families who are new to the process of addressing a loved one’s addiction often use the words “intervention” and “treatment” interchangeably. It is an understandable confusion. Both are part of the path toward recovery. Both involve professionals. But they are not the same thing, and confusing them can delay getting the right kind of help […]