by Clear Path Intervention
Share
by Clear Path Intervention
Share

California does not fit the story most people carry in their heads about the overdose crisis. It is, by prescribing measures, one of the most cautious states in the country. It also contains some of the most visible, concentrated drug crises in America. Both things are true at once, and holding them together is the only way to understand what is actually happening, and what it means for a family trying to help someone here.
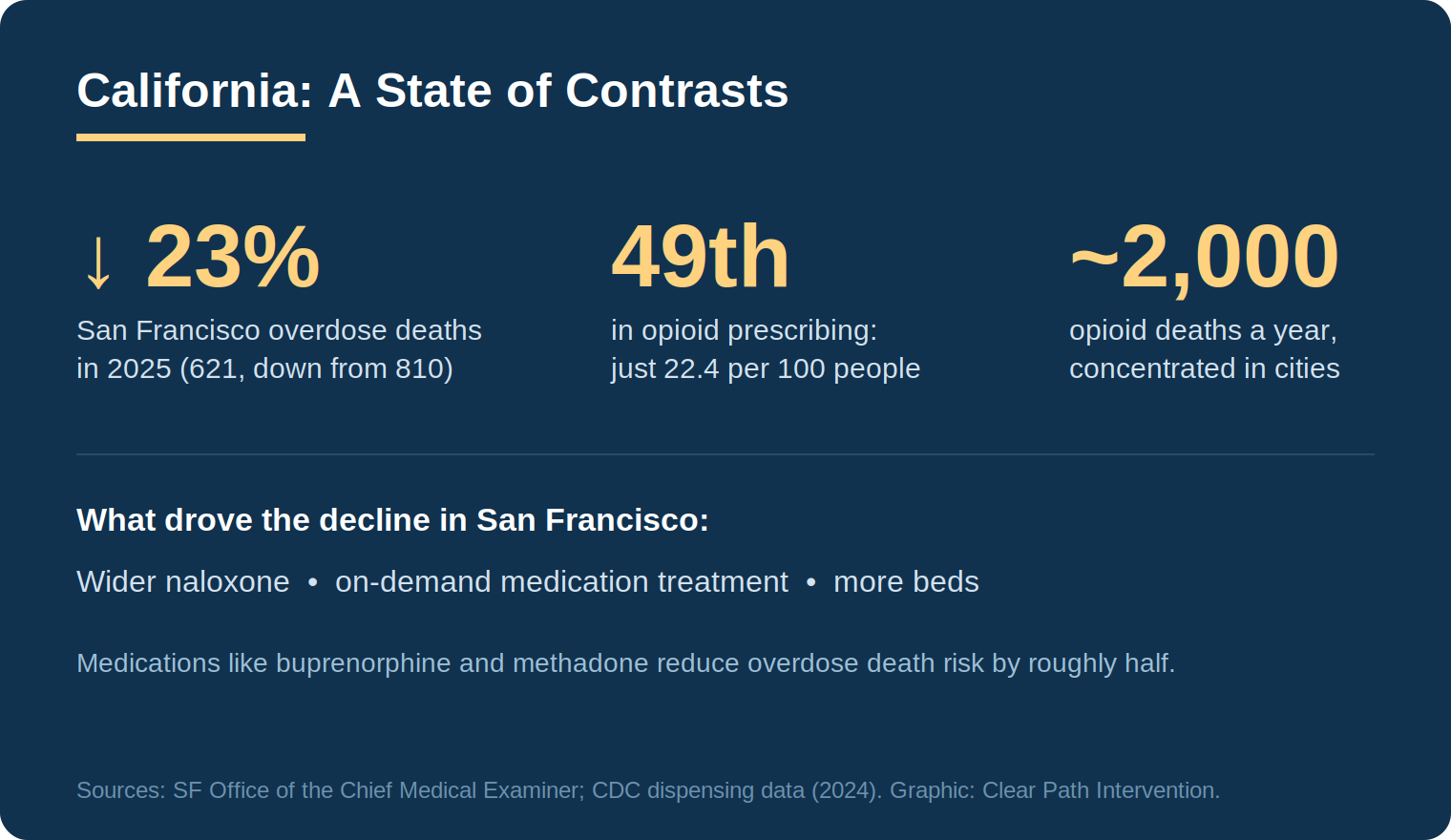
The most encouraging recent number comes from San Francisco, long treated as shorthand for the fentanyl emergency. In January 2026, city officials reported that accidental overdose deaths fell to 621 in 2025, down more than 23 percent from the 2023 peak of 810, the lowest total in five years. Progress that was not inevitable. It happened because the city expanded specific, evidence-based tools, which is the part of the story most worth understanding.
The contrast, explained
Start with prescribing. CDC data for 2024 places California near the very bottom of the national table, with an opioid dispensing rate of about 22.4 prescriptions per 100 people, second-lowest in the country and far below states like Arkansas and Alabama. By that measure, California is doing well. Fewer prescriptions historically means fewer people introduced to opioids through the medical system.
Yet California still loses roughly two thousand people a year to opioid-related overdose, and the crisis is intensely concentrated in specific neighborhoods and populations rather than spread evenly. This is the contrast. The state’s problem is driven far less by the prescription pipeline that defines the rural South, and far more by an illicit street supply of fentanyl that is cheap, potent, and concentrated in urban centers. Understanding that distinction matters, because it points to different solutions. In California, the lever is rarely prescribing reform. It is reaching people already entangled in the illicit supply and getting them into treatment.
Why San Francisco’s numbers came down
The San Francisco decline is instructive precisely because the city did not stumble into it. Officials credited the drop to a deliberate expansion of evidence-based interventions: wider distribution of the overdose-reversal medication naloxone, more residential and treatment beds, and on-demand access to medication for opioid use disorder. The city built a program allowing people who use fentanyl to reach a medical provider and begin buprenorphine, a medication that, along with methadone, reduces the risk of overdose death by roughly half.
That last point is worth dwelling on, because it is one of the most robust findings in addiction medicine and one of the most misunderstood by families. Medication for opioid use disorder is not, as the old stigma held, trading one drug for another. It is the standard of care, and the research is consistent that it keeps people alive and in recovery far better than abstinence-only approaches for opioid addiction. A family weighing options for a loved one should know that medication-based treatment is evidence-based, not a compromise.
How addiction shows up across California
California is too large and varied to describe in one breath. The interventionists who work with families across California see distinct regional realities.
San Francisco and the Bay Area
The most visible street-level fentanyl crisis in the state has centered on neighborhoods like the Tenderloin, where the supply is unusually cheap and the public nature of use draws national attention. The recent decline shows the trend is not fixed. For families here, the surrounding treatment infrastructure is among the most developed in the country, which is an advantage worth using.
Los Angeles
As the center of a vast treatment industry, the Los Angeles area presents families with both abundant options and a specific risk: the quality of programs varies enormously, and some referral arrangements are shaped by financial relationships rather than clinical fit. This is the place to ask hard questions about how a treatment recommendation is being made. Reputable guidance is driven by what suits the patient, not by who pays a referral fee.
San Diego
Its position near the border places the San Diego region close to a major fentanyl trafficking corridor, with the steady availability that proximity brings. The counterfeit-pill problem, pills pressed to look like legitimate medication but containing unpredictable amounts of fentanyl, is well represented across Southern California.
Sacramento and the Central Valley
Inland, the Sacramento region and the broader Central Valley face a heavier methamphetamine presence alongside fentanyl, and thinner treatment resources than the coastal metros. The polysubstance pattern, more than one drug at once, is the norm rather than the exception.
Recognizing when it is time to act
Because California’s crisis is so concentrated and so often invisible from the outside, families frequently wonder whether what they are seeing is serious enough to warrant action. It is a fair question, and the honest answer is that waiting for certainty usually means waiting too long. There is rarely a single dramatic moment that announces an addiction. More often there is a slow accumulation of changes that, taken together, tell the story.
Some of the more reliable signs are behavioral rather than physical. Withdrawal from family and longtime friends. A new and secretive social circle. Money that goes missing, or unexplained financial trouble. Declining performance at work or school in someone who previously managed both. A loved one who becomes defensive or evasive when asked ordinary questions about their day. Physical signs, such as changes in sleep, weight, or appearance, tend to appear too, but often later than the behavioral ones, which is why families who wait for visible deterioration frequently act late.
It also helps to understand why a struggling person so rarely raises the issue themselves. The same brain changes that drive continued use impair insight into the problem. This is not denial in the ordinary sense of stubbornness. It is a genuine difficulty perceiving the situation accurately, which is part of why the people around a person often see the problem before the person does.
The fentanyl era has also compressed the timeline families have to work with. In earlier decades, a developing addiction might progress over years, leaving room to notice and respond. Today, because the illicit supply is so potent and unpredictable, the gap between occasional use and a fatal outcome can be a single pill. That change is why professionals now encourage families to act on early concern rather than waiting for the problem to mature. The old timeline assumed survival. The current one does not. When several of these signs cluster together, that is usually the moment to seek guidance.
A note on trust, and how families fit in
The treatment-industry concern raised above deserves its own moment, because it shapes outcomes more than families realize. Some intervention providers and referral services accept compensation from the treatment centers they recommend, a practice that can quietly steer a loved one toward whoever pays rather than whoever fits. Families are entitled to ask anyone they work with whether that is the case, and to expect placements based on clinical need. It is a fair question to put to any professional.
Within a system as developed as California’s, the family’s role is not to replace the infrastructure but to do the one thing the infrastructure cannot: reach the specific person who has not yet walked through the door. The evidence on family involvement is encouraging here. Structured, prepared approaches such as the research-supported CRAFT model, documented in the clinical literature gathered by SAMHSA, engage a meaningful share of previously treatment-resistant people by coaching the family in how to communicate rather than how to confront. The science of why this works is the same everywhere. Addiction alters the brain circuits involved in motivation and judgment, a process detailed in NIDA’s research on drug misuse and addiction, which is why a loved one often cannot accurately weigh their own risk and why the people around them end up carrying part of that judgment.
California’s contrasts, taken together, hold a genuinely hopeful lesson. The San Francisco decline demonstrates that the tools work when they are deployed. The state’s low prescribing rate shows that prevention upstream is possible. And the concentration of the crisis in specific places means the problem, while severe, is not beyond the reach of focused, evidence-based response. For a family, the practical takeaway is that effective treatment exists and is reachable. The task is getting a loved one to it.
For families in California specifically, early guidance carries an added benefit. Because the state’s treatment landscape is so large and uneven, knowing what to look for in a program, and what questions to ask about how a referral is made, is as important as the decision to act. The best time to learn those things is before a crisis, not in the middle of one.
For continuing context, the CDC overdose prevention center tracks national and state data, and the California Department of Public Health maintains a state overdose dashboard. Anyone in immediate crisis can reach the SAMHSA National Helpline at 1-800-662-HELP or dial 988.
HELP IS AVAILABLE
Do You Have a Loved One Struggling with Addiction or Mental Health Issues?

There is a particular kind of exhaustion that comes from loving someone whose drug addiction has taken over their life. You have had the conversations. You have made the threats — and not followed through. You have set boundaries — and let them slip. You have searched online at 2 a.m. and closed the laptop […]

When a family is in crisis — when a loved one’s addiction has reached the point where something has to happen — the pressure to act quickly can make it hard to think clearly about who to call. The intervention field is largely unregulated. Anyone can call themselves an interventionist. The quality of services ranges […]

Families who are new to this process often have a narrow picture of what a professional intervention service involves. A specialist shows up, talks to the family for a bit, sits in the room during the conversation, and leaves. That picture is missing most of what actually happens — and most of what makes the […]

Families who are new to the process of addressing a loved one’s addiction often use the words “intervention” and “treatment” interchangeably. It is an understandable confusion. Both are part of the path toward recovery. Both involve professionals. But they are not the same thing, and confusing them can delay getting the right kind of help […]