by Clear Path Intervention
Share
by Clear Path Intervention
Share
")
The national story about overdose in 2026 is, for once, a hopeful one. Deaths have fallen for several years running. Arizona is the exception to that story. While the rest of the country has been recording its first sustained relief from the fentanyl crisis, Arizona has been moving in the opposite direction, and the gap is not small.
For families in the state, this is more than a statistical curiosity. It means the reassurance other Americans are reading in the headlines does not apply to them in the same way. The danger in Arizona is not receding. By the most recent count, it is intensifying. Understanding why requires looking past the national average to the specific forces shaping this one state.
An outlier, quantified
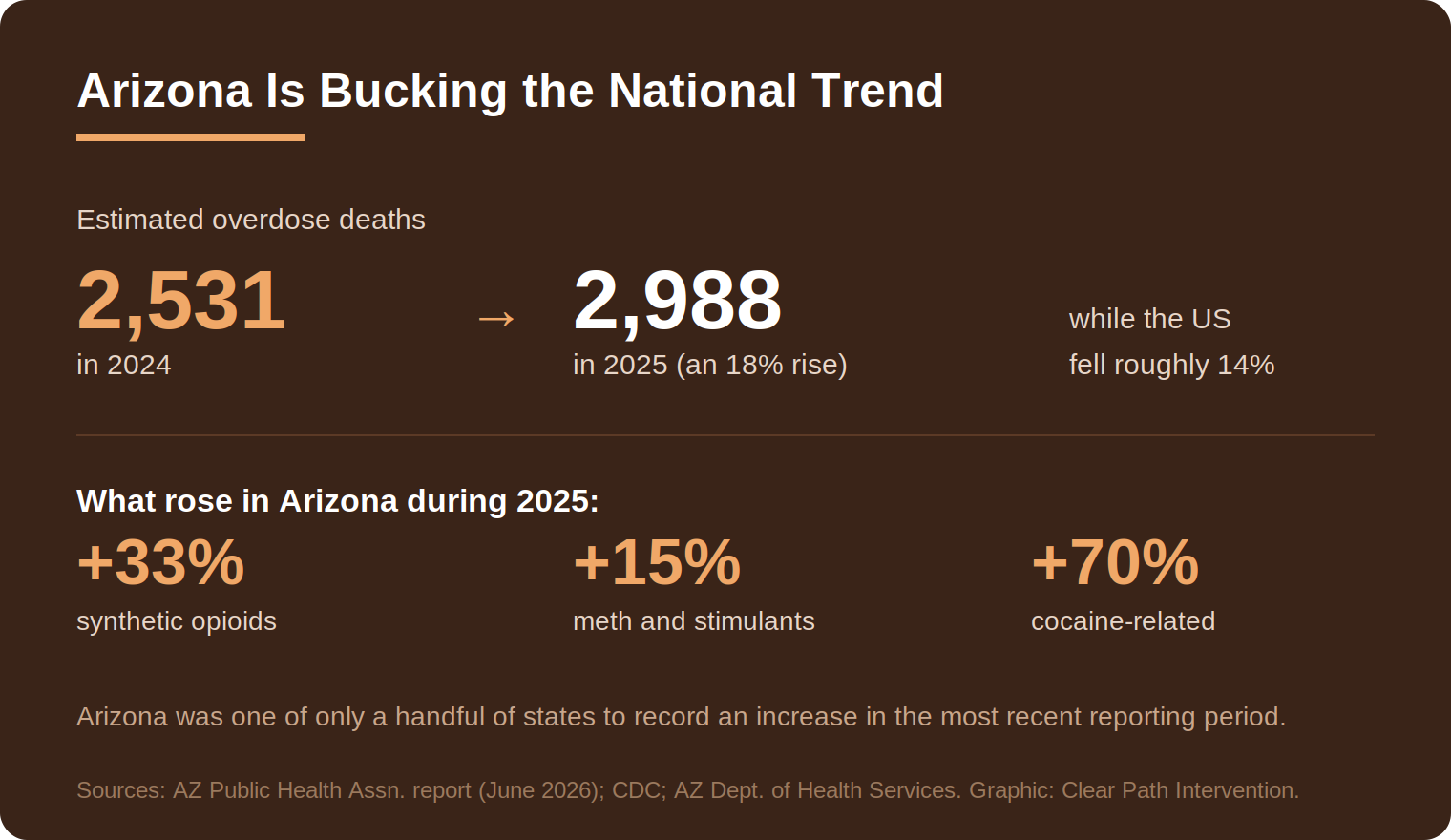
The clearest recent accounting comes from the Arizona Public Health Association, which in June 2026 published a special report examining why the state is diverging from the country. The findings are stark. Estimated overdose deaths in Arizona rose about 18 percent, from roughly 2,531 in 2024 to 2,988 in 2025, even as national deaths fell by nearly 14 percent over a comparable window. The increases were broad. Deaths involving synthetic opioids, mostly fentanyl, climbed by roughly a third. Methamphetamine and other stimulant deaths rose more than 15 percent. Cocaine-related deaths jumped almost 70 percent.
This was not a one-report anomaly. Earlier in 2026, the Arizona Capitol Times reported that for the twelve-month period ending in September 2025, Arizona was one of only five states to record an increase in overdose deaths, and had the largest increase of any state in the country. National fentanyl deaths fell about 31 percent over that period. Arizona’s rose about 30 percent. The lines were not just diverging. They were pointing in opposite directions at nearly the same speed.
Why Arizona, and why now
No single factor fully explains an outlier, but the analyses converge on geography as a primary driver. Arizona shares a long border with Mexico, and the state sits astride one of the most heavily trafficked corridors for illicitly manufactured fentanyl entering the United States. Law enforcement seizures at Arizona ports of entry have run into the millions of pills, a scale of supply that helps explain why local availability has not eased in step with the national trend.
The state’s response has leaned heavily on enforcement. Prosecutors in Maricopa County have begun applying a newer state law that allows fentanyl dealers to be charged more severely when their drugs cause a death, and the county attorney’s office has described its proximity to the border as placing it at the center of the crisis. Whatever one makes of the policy approach, the underlying fact it responds to is the same: the supply reaching Arizona communities is large, cheap, and increasingly contaminated with multiple substances at once.
That contamination is the thread connecting the rising numbers across drug categories. As the Arizona Department of Health Services has documented, the overwhelming majority of the state’s opioid overdose deaths are accidental, and fentanyl now turns up mixed into pills and powders sold as something else. A person who believes they are using cocaine, or a counterfeit prescription pill, may be ingesting fentanyl without knowing it. The 70 percent rise in cocaine-related deaths is far less puzzling once that cross-contamination is understood.
The counterfeit pill problem, explained
To make sense of Arizona’s numbers, it helps to understand the product moving through the state. The illicit fentanyl driving the crisis is largely pressed into counterfeit pills built to look like legitimate prescription medication: fake oxycodone, fake alprazolam, fake stimulants. The Drug Enforcement Administration has warned through public education campaigns such as One Pill Can Kill that a large share of seized counterfeit pills carry a potentially lethal dose of fentanyl, and that a contaminated pill cannot be told apart from a genuine one by sight, taste, or smell.
The manufacturing pipeline explains the unpredictability. Precursor chemicals are produced overseas, the pills are pressed in clandestine labs, and the finished product moves north in volume. Because the pressing is crude, the amount of fentanyl in any single pill varies enormously from one to the next. One pill in a batch may contain a survivable amount. The next may not. This is the mechanism behind a pattern Arizona families describe over and over: a person who had used for a long time, seemingly stable, dies suddenly from what looked like an ordinary dose. The dose was not ordinary. It simply could not be seen.
The same dynamic explains the otherwise puzzling rise in cocaine and stimulant deaths. When fentanyl contaminates the wider drug supply, people who never intended to use an opioid are exposed to one anyway, often with no tolerance and no warning. Methamphetamine deserves separate mention, given its sharp rise in the state. Unlike opioids, stimulant addiction has no approved medication comparable to the treatments available for opioid use disorder, which makes structured behavioral treatment and family support the central tools. Meth also tends to produce more visible psychological symptoms, including paranoia and prolonged sleeplessness, which can make the conversation with a loved one harder and the case for experienced guidance stronger.
What rising numbers change for families
It is worth being precise about what this means and what it does not. A rising statewide death count does not mean recovery is less possible in Arizona than elsewhere. Treatment works the same way in Phoenix as it does in cities where the numbers are falling. What changes is the risk environment surrounding a person who has not yet entered treatment. In a state where the supply is growing more lethal rather than less, the cost of waiting is higher.
This connects to the science of how addiction operates. The National Institute on Drug Abuse describes substance use disorder as a chronic medical condition that alters the brain circuits governing reward, stress, and self-control, as detailed in NIDA’s research on the science of addiction. One practical consequence is that the affected person often cannot accurately weigh their own risk, even when the danger is escalating around them. They are not ignoring the rising numbers out of stubbornness. The condition itself impairs the very judgment that would let them respond to the warning.
That is the gap families step into. When a loved one cannot assess their own situation, the people around them have to do some of that assessing on their behalf, and then act on it. In an environment as dangerous as Arizona’s current one, that responsibility arrives sooner than families expect.
How the crisis varies across Arizona
The interventionists who work with families across Arizona see the statewide trend express itself differently from one region to the next.
Phoenix and Maricopa County
As the population center and the focus of the state’s enforcement efforts, the Phoenix metro carries the largest share of the state’s overdose burden and also the most extensive treatment infrastructure. For families here, services are reachable, but the same density of supply that makes the metro a distribution hub keeps exposure high.
Tucson and the border region
Closer to the international border, the Tucson area sits near the ports of entry where large fentanyl seizures are routine. The proximity that drives the seizures also drives availability, and the counterfeit-pill problem is especially acute in the southern part of the state.
Mesa and Scottsdale
In the eastern and northern suburbs, families in the Mesa and Scottsdale communities often describe an addiction that began with prescription medication and stayed hidden behind comfortable circumstances. Affluence is not protection. It frequently just delays the point at which a family treats the problem as urgent.
Flagstaff and northern Arizona
In the high country and across the Four Corners region, families near Flagstaff contend with rural distances and, in tribal communities, some of the steepest overdose disparities in the country. Regional reporting has documented rising synthetic-opioid deaths across the Four Corners even as the nation improved, a reminder that the statewide average can hide pockets where the trend is worse still.
Reading the Arizona numbers without despair
There is a temptation, looking at a chart that points the wrong way, to conclude that nothing is working. That reading is not supported by the evidence. The national decline demonstrates that the tools exist and that they save lives when deployed. Wider naloxone access, fentanyl test strips, and timely entry into treatment have measurably bent the curve in most of the country. Arizona’s outlier status is better understood as a supply problem layered over those tools, not as proof that the tools fail.
For a family, the useful takeaway is narrower and more actionable. The statewide trend is a description of the environment, not a prediction about any one person. Recovery remains entirely possible. What the 2026 data adds is urgency, by establishing that in Arizona specifically, the window in which a loved one is exposed to the supply is more dangerous this year than last. That is a reason to take warning signs seriously and to treat the question of getting someone into care as time-sensitive rather than indefinite.
For continuing context, the CDC overdose prevention center tracks national and state provisional data, and the Arizona Department of Health Services publishes state surveillance reports. Anyone in immediate crisis can reach the SAMHSA National Helpline at 1-800-662-HELP or dial 988.
HELP IS AVAILABLE
Do You Have a Loved One Struggling with Addiction or Mental Health Issues?

California does not fit the story most people carry in their heads about the overdose crisis. It is, by prescribing measures, one of the most cautious states in the country. It also contains some of the most visible, concentrated drug crises in America. Both things are true at once, and holding them together is the […]

Every state’s addiction story has a starting point. In Arkansas, more than in almost anywhere else in the country, that story began at the pharmacy counter. For years the state has led or nearly led the nation in how many opioid prescriptions its doctors write, and that history still shapes the crisis families face today. […]

In most of the country, the question facing a family is whether a loved one will accept treatment. In Alaska, there is a second question stacked on top of the first. If they say yes, where exactly do they go, and how do they get there before the willingness fades? That second question is not […]

For the first time in nearly a decade, Alabama is recording fewer overdose deaths than it did the year before. That is worth saying plainly, because families living inside the addiction crisis rarely hear good news. In January 2026, state outlets reported that more than 900 Alabamians died of drug overdoses in the most recent twelve-month […]