by Clear Path Intervention
Share
by Clear Path Intervention
Share

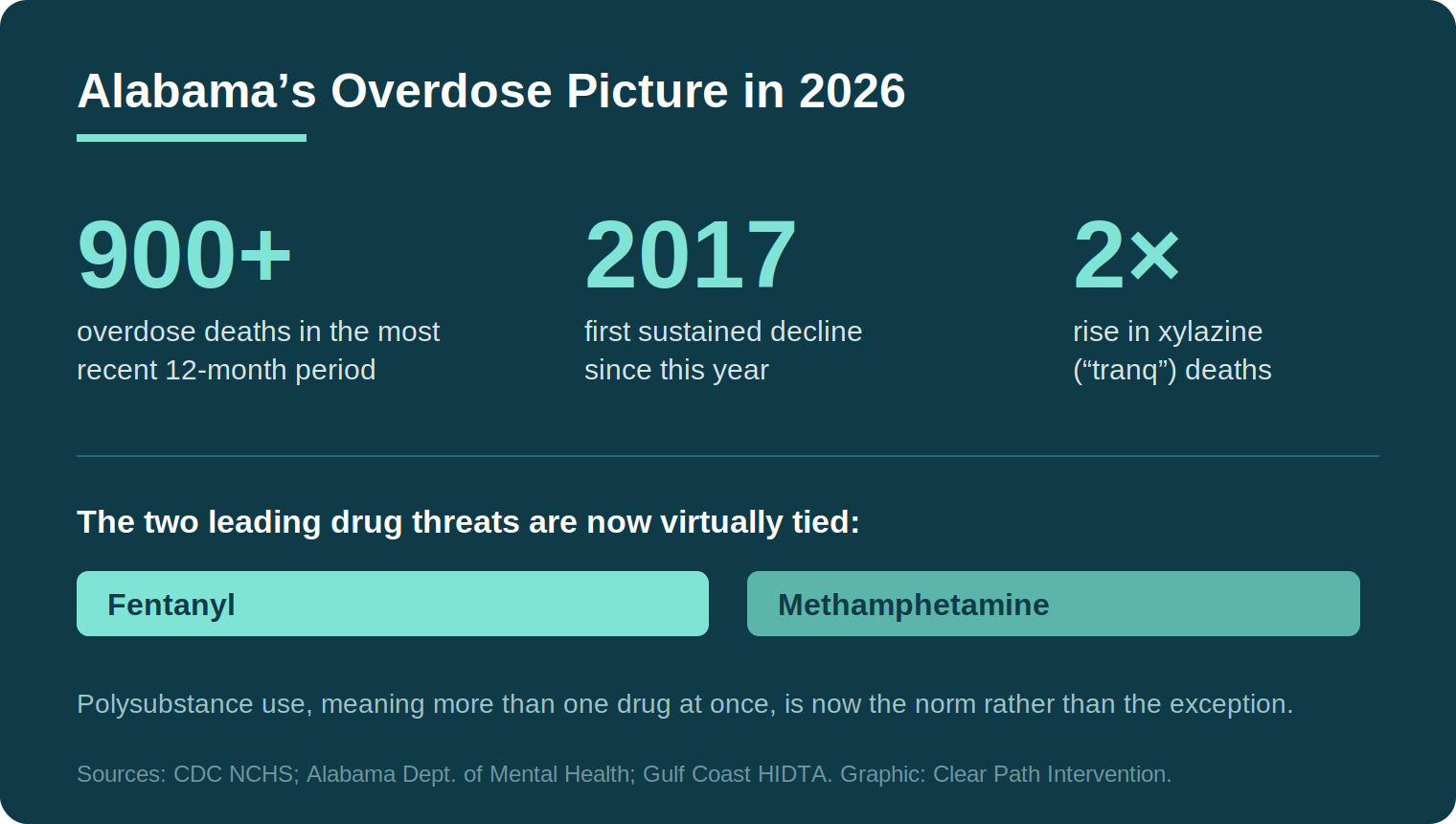
For the first time in nearly a decade, Alabama is recording fewer overdose deaths than it did the year before. That is worth saying plainly, because families living inside the addiction crisis rarely hear good news. In January 2026, state outlets reported that more than 900 Alabamians died of drug overdoses in the most recent twelve-month period, down from the state’s 2023 fentanyl peak. Progress. Real and measurable.
And yet the counselors and clinicians quoted alongside those numbers kept returning to the same uncomfortable point. The supply is more dangerous than it has ever been. Fewer people are dying, but the people still using are playing a game with worse odds than the families around them understand. Understanding why that is true, and what it changes, is the purpose of this article.
What the data shows, and what it leaves out
The national context matters here. According to the CDC’s National Center for Health Statistics, drug overdose deaths across the United States fell sharply between 2023 and 2024, the first meaningful decline in years, a trend documented in the agency’s overdose mortality data briefs. Researchers attribute much of that improvement to the wider availability of naloxone, expanded access to medication for opioid use disorder, and a possible shift in the illicit supply itself.
Alabama followed that national curve, if more modestly. The state’s own Department of Mental Health has documented the decline while flagging the trends hiding underneath it. Fentanyl is increasingly mixed with methamphetamine and with sedatives such as xylazine, an animal tranquilizer with no approved human use that does not respond to naloxone. The Gulf Coast High Intensity Drug Trafficking Area program has reported that methamphetamine and fentanyl now sit nearly tied as the state’s primary drug threats. Two crises, braided together.
So the headline and the reality diverge. A falling death count reflects better rescue and better treatment access at the population level. It says very little about whether any one person’s daily exposure has gotten safer. It has not. A counterfeit pill purchased today is more likely to contain an unpredictable mix of substances than it was three years ago, which is precisely why overdose reversal has become harder in some cases even as the broader numbers improve.
Why a statewide decline does not mean your loved one is safer
This is the part families find hardest to hold onto, and it is where the science is clearest. Addiction is not a measure of willpower or character. The National Institute on Drug Abuse describes substance use disorder as a chronic, treatable medical condition that alters the brain’s reward, stress, and self-control circuitry, a framing laid out across NIDA’s research on the science of addiction. Those changes are real, physical, and persistent. They help explain something families witness constantly and rarely have language for: the person they love can recognize the danger intellectually and still be unable to stop.
That neurological reality is the reason a downward statewide trend offers a struggling individual so little protection. Population data describes thousands of people. Your loved one is one nervous system, one supply chain, one bad batch. The brain changes that drive continued use do not read the CDC’s annual report. They keep operating regardless of which direction the chart is moving.
Which leads to a difficult but important conclusion. The improvement Alabama is seeing happened because people reached treatment, not because the danger receded on its own. The lever that moves an individual’s odds is the same lever that moved the state’s: getting the person into care. Earlier rather than later.
How addiction is showing up across Alabama
Alabama is not a single story. The pressures on a family in a downtown high-rise differ from those on a family two hours into the country, and the resources within reach differ too. The interventionists who work with families across Alabama see those regional differences play out in distinct ways.
Birmingham
As the state’s largest metro and home to one of the South’s premier academic medical systems, the Birmingham area carries both the heaviest overdose burden in the state and its deepest bench of treatment resources. For families here the advantage is proximity. Quality care is often a short drive away. The complicating factor is that easy access to an urban supply can make the progression fast, which narrows the window between the first serious warning sign and a crisis that lands someone in a Jefferson County emergency department.
Montgomery
The River Region felt the synthetic-opioid surge acutely. At the height of the crisis, local prosecutors described overdose cases arriving on a near-weekly basis. For families in and around Montgomery, the recent statewide decline is genuine cause for some optimism. The synthetic supply, however, remains the central danger, and the polysubstance pattern documented statewide is well represented in central Alabama.
Mobile and the Gulf Coast
Sitting on a trafficking corridor tracked by the Gulf Coast HIDTA program, the Mobile region sees a steady movement of fentanyl and methamphetamine through the port and along Interstate 10. Co-use of fentanyl and methamphetamine is increasingly common rather than exceptional, a combination that complicates both overdose risk and the clinical picture a family is dealing with.
Huntsville
The Rocket City’s rapid growth, powered by its aerospace and defense workforce, has brought new prosperity and new pressures. Families in the Huntsville area often describe a loved one whose addiction is concealed behind a high-functioning professional life: the security-cleared engineer, the well-regarded contractor, the parent who has never missed a deadline. High function is not the same thing as safety. It tends to delay the moment a family feels they have permission to act.
What the evidence says about intervention
Because families often arrive at the idea of a formal intervention through television, it helps to separate the dramatized version from the clinical one. There is no single method called “intervention.” There are several structured, studied approaches, and they differ in meaningful ways.
The Johnson Model, the approach most people picture, gathers a prepared group to present concerns and a clear request to enter treatment. Newer family-systems models such as ARISE and the research-supported CRAFT approach (Community Reinforcement and Family Training) emphasize a more gradual, less confrontational process and place heavy weight on coaching the family rather than confronting the individual. CRAFT in particular has accumulated a notable evidence base. Controlled studies have found that training family members in specific communication and reinforcement strategies engages a substantial share of previously treatment-resistant loved ones into care, often at higher rates than traditional confrontational methods. The clinical literature compiled by SAMHSA and by NIDA consistently points in the same direction: family involvement improves outcomes, and how that involvement is structured matters.
What unites the credible approaches is preparation. A useful intervention is not a surprise ambush. It is a planned conversation built on a shared, non-negotiable message, with a treatment placement arranged in advance so that a yes can be acted on the same day rather than lost to a forty-eight-hour delay. In practice, the families who fare best tend to spend significant time before the conversation learning how addiction actually works, aligning on what they will and will not do, and rehearsing. The conversation is the visible part. The work is mostly invisible.
It is also worth naming a trust issue that sits underneath this whole field. Some referral services and intervention providers accept compensation from the treatment centers they recommend, which can quietly distort where a loved one is sent. Families are entitled to ask anyone they work with whether that is the case, and to expect placements driven by clinical fit rather than financial relationships.
The window that families can actually control
Here is the throughline. Alabama’s numbers came down because people got into treatment, and the supply that remains is more lethal and less predictable than the one that produced the 2023 peak. Those two facts, taken together, are not a contradiction. They are an argument for acting inside the window a family can influence, rather than waiting for a crisis to force the issue.
The familiar instinct is to wait for rock bottom, on the theory that a person has to want recovery before help can work. The research complicates that belief. Engagement and motivation frequently follow entry into treatment rather than preceding it, which is part of why early, structured family action is associated with better outcomes than passive waiting. Rock bottom, in too many Alabama families, has turned out to be a funeral.
None of this requires panic. It requires accurate information, which is the one thing the headlines tend to flatten. The decline is real. So is the danger. Holding both at once, without letting the good news become a reason to look away, is the most useful thing a family watching a loved one can do with the 2026 data.
For ongoing national context, the CDC’s overdose prevention center and the NIDA overdose statistics are both regularly updated. Anyone in immediate crisis can reach the SAMHSA National Helpline at 1-800-662-HELP or dial 988.
HELP IS AVAILABLE
Do You Have a Loved One Struggling with Addiction or Mental Health Issues?

California does not fit the story most people carry in their heads about the overdose crisis. It is, by prescribing measures, one of the most cautious states in the country. It also contains some of the most visible, concentrated drug crises in America. Both things are true at once, and holding them together is the […]

Every state’s addiction story has a starting point. In Arkansas, more than in almost anywhere else in the country, that story began at the pharmacy counter. For years the state has led or nearly led the nation in how many opioid prescriptions its doctors write, and that history still shapes the crisis families face today. […]

The national story about overdose in 2026 is, for once, a hopeful one. Deaths have fallen for several years running. Arizona is the exception to that story. While the rest of the country has been recording its first sustained relief from the fentanyl crisis, Arizona has been moving in the opposite direction, and the gap […]

In most of the country, the question facing a family is whether a loved one will accept treatment. In Alaska, there is a second question stacked on top of the first. If they say yes, where exactly do they go, and how do they get there before the willingness fades? That second question is not […]