by Clear Path Intervention
Share
by Clear Path Intervention
Share
")
Geography has made Atlanta one of the great commercial crossroads of the American South, a hub where interstates, rail, and the world’s busiest airport converge. That same centrality has a darker dimension. For the illicit drug trade, metro Atlanta functions as a distribution hub for much of the Southeast, and the consequences ripple outward across Georgia and into neighboring states. Understanding that role is key to making sense of the state’s overdose picture, which in 2026 is improving and dangerous at the same time.
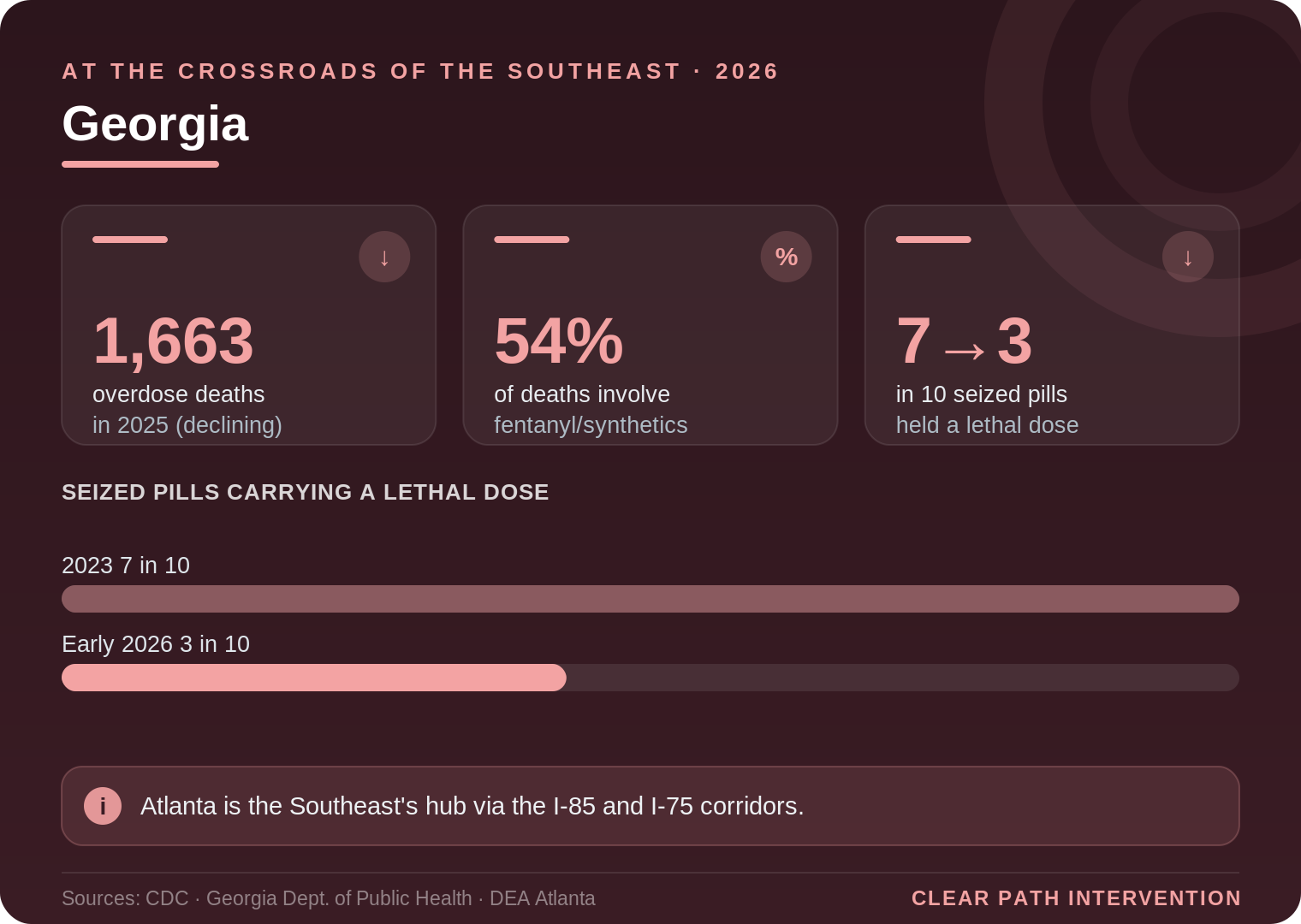
The improvement is real. According to data from the Atlanta-based Centers for Disease Control and Prevention, 1,663 people died of overdoses in Georgia in 2025, a significant decline, though the drop ran slightly below the national average. Synthetic opioids, chiefly fentanyl, remained the largest single contributor. A state moving in the right direction, but not out of danger, and still shaped by its position at the center of the region’s drug routes.
What the Georgia data shows
Georgia’s overall overdose death rate has historically run somewhat below the national average, but the trajectory tells the more important story. The Georgia Department of Public Health traces the modern crisis through familiar waves: a rise driven by prescription opioids beginning around 2010, a shift toward heroin and fentanyl from 2013, and a sharp acceleration after 2020 as fentanyl began contaminating stimulants like cocaine and methamphetamine. Today, fentanyl and other synthetic opioids are involved in roughly 54 percent of the state’s overdose deaths.
There is encouraging movement on the enforcement side as well. In January 2026, the DEA’s Atlanta Division launched a regional campaign against fentanyl, and officials reported that the share of seized counterfeit pills containing a potentially lethal dose had fallen from about seven in ten in 2023 to roughly three in ten by early 2026. That is meaningful progress in the supply. But the same officials were careful to stress that fentanyl remains lethal in tiny amounts, and that traffickers continually adapt their methods, concealing drugs in increasingly creative ways as they move product through the region.
The hub effect, and why it matters for families
Atlanta’s role as a distribution point has a direct bearing on what families across Georgia experience. When a metro becomes a hub, the supply is not only abundant there but radiates outward along the interstate corridors, the I-85 and I-75 routes that connect Atlanta to the rest of the South. This is part of why counterfeit pills and fentanyl-contaminated stimulants reach communities far from the city, and why a problem that looks like an Atlanta issue is really a statewide one.
The contamination of stimulants deserves particular emphasis, because it has changed who is at risk. A person who uses cocaine recreationally, who would never knowingly touch an opioid, can now be exposed to fentanyl without any awareness of it. Georgia’s own surveillance has documented clusters of this kind, including a notable counterfeit-pill overdose cluster in Macon years ago that foreshadowed the broader pattern. The result is that the line between casual stimulant use and a fatal opioid overdose has blurred, and families whose loved one uses any illicit substance, not only opioids, have reason for concern.
How the crisis looks across Georgia
The interventionists who work with families across Georgia encounter the state’s regions as distinct settings, each with its own pressures.
Atlanta
As the population center and the regional hub, the Atlanta metro carries both the largest share of the state’s overdose burden and its deepest concentration of treatment resources. Proximity to the supply accelerates the progression of addiction, but proximity to quality care is an advantage families can use if they act before a crisis forces the issue.
Savannah and the coast
A historic port city, the Savannah area sits on a coastal trafficking corridor, and federal reporting has described traffickers adapting their concealment methods to move drugs through southeast Georgia. The same polysubstance pattern seen statewide is well represented along the coast.
Columbus and middle Georgia
Home to a large military community at Fort Moore, the Columbus region sees the particular intersection of addiction with service-related trauma and chronic pain, where co-occurring conditions are common and a thorough assessment matters.
Augusta and Athens
Georgia’s mid-size metros face their own versions of the crisis. Augusta, anchored by a major medical center, and Athens, shaped by the University of Georgia, contend respectively with the access patterns of a regional hub and the young-adult risks of a college town, where a single counterfeit pill can carry a fatal dose.
When occasional use becomes lethal
One of the most important shifts for Georgia families to understand is how the contamination of the drug supply has changed who is at risk. In an earlier era, the people most likely to die of an overdose were those with long, heavy patterns of opioid use, who had developed both dependence and a degree of tolerance. That is no longer the case. Because fentanyl is now pressed into counterfeit pills and mixed into stimulants like cocaine, a person who uses only occasionally, and who has no tolerance, can die from a single dose they did not know contained an opioid.
This is the mechanism behind the stories that bewilder families: a young person who experimented at a party, a student who bought what they believed was a prescription stimulant to study, an occasional cocaine user who never intended to touch an opioid. The Drug Enforcement Administration has warned repeatedly that counterfeit pills cannot be distinguished from genuine medication by sight, and that a meaningful share contain a potentially lethal amount of fentanyl. The danger is no longer confined to people with a visible, long-standing addiction.
For families, this widens the circle of concern in a useful way. It means that warning signs in a loved one who uses any illicit substance, not only opioids, deserve to be taken seriously. Behavioral changes such as withdrawal from family, a new and secretive social circle, financial trouble, or declining performance at work or school are worth attention regardless of which drug a family believes is involved, because the supply has blurred the lines between them.
It also reframes what acting early means. A family does not need to wait for the classic picture of addiction to justify seeking guidance. In a state where Atlanta’s hub status keeps the contaminated supply flowing outward, the prudent response to genuine concern is to seek informed advice promptly rather than waiting for a pattern to harden into a crisis.
What the evidence says about getting someone into care
The blurring of stimulant and opioid risk in Georgia strengthens the case for acting on concern rather than waiting for certainty. A family that assumes their loved one is safe because they only use cocaine, or only use pills bought from a friend, is operating on an outdated map of the supply. The contamination has made occasional use lethal in a way it was not a decade ago.
When families decide to act, the approaches with the strongest evidence share a reliance on preparation over confrontation. The Johnson Model assembles a prepared group to express concern and offer a clear route to care. Family-systems methods such as ARISE, and the research-supported CRAFT approach (Community Reinforcement and Family Training), place greater weight on coaching the family in communication and positive reinforcement, and CRAFT in particular has been found in controlled studies to engage a substantial share of previously resistant people. The clinical guidance compiled by SAMHSA consistently finds that structured family involvement improves outcomes.
The science underneath this matters because it reframes the problem accurately. Addiction alters the brain circuits that govern judgment, reward, and self-control, a process documented in NIDA’s research on drug misuse and addiction, which is part of why a loved one frequently cannot weigh their own risk accurately. Someone has to help carry that judgment, and a prepared family is well positioned to do it. A useful plan also arranges a treatment placement in advance, so a yes can be honored immediately rather than lost to delay, and given the polysubstance reality, an honest assessment of what a person is actually using is a sensible first step.
Georgia’s improving numbers and its falling share of lethal counterfeit pills are real gains, and the people working to achieve them deserve recognition. But the state’s position at the crossroads of the Southeast means the supply will keep coming, and keep changing. For a family, the useful response is not to wait for the statewide trend to feel safe, but to recognize that the trend describes the environment, not their loved one, and that the path into care remains open and effective regardless of which way the chart is pointing.
For continuing context, the CDC overdose prevention center and the Georgia Department of Public Health both publish regularly updated data. Anyone in immediate crisis can reach the SAMHSA National Helpline at 1-800-662-HELP or dial 988.
HELP IS AVAILABLE
Do You Have a Loved One Struggling with Addiction or Mental Health Issues?

Florida is posting some of the most encouraging overdose numbers in the country. It is also a state with one of the most complicated relationships to the addiction crisis in America, from the pill mills that helped ignite the national epidemic to a treatment industry that has, at times, exploited the very people it promised […]

Delaware is one of the smallest states in the country, and for years it carried one of the heaviest overdose burdens, measured against its size. By the most recent national comparisons, Delaware ranked second only to West Virginia in its rate of fentanyl-involved overdose deaths. A small population, an outsized loss. That history is what […]

For most of the country, 2025 brought the first real relief from the fentanyl crisis in years. Colorado got a different report. While national overdose deaths fell sharply, Colorado became one of a small group of states where the numbers turned back upward, and its largest city recorded one of its worst years on record. […]

California does not fit the story most people carry in their heads about the overdose crisis. It is, by prescribing measures, one of the most cautious states in the country. It also contains some of the most visible, concentrated drug crises in America. Both things are true at once, and holding them together is the […]