by Clear Path Intervention
Share
by Clear Path Intervention
Share
")
Florida is posting some of the most encouraging overdose numbers in the country. It is also a state with one of the most complicated relationships to the addiction crisis in America, from the pill mills that helped ignite the national epidemic to a treatment industry that has, at times, exploited the very people it promised to help. Both of those facts deserve a place in any honest account of where Florida stands in 2026, especially for a family trying to find trustworthy help here.
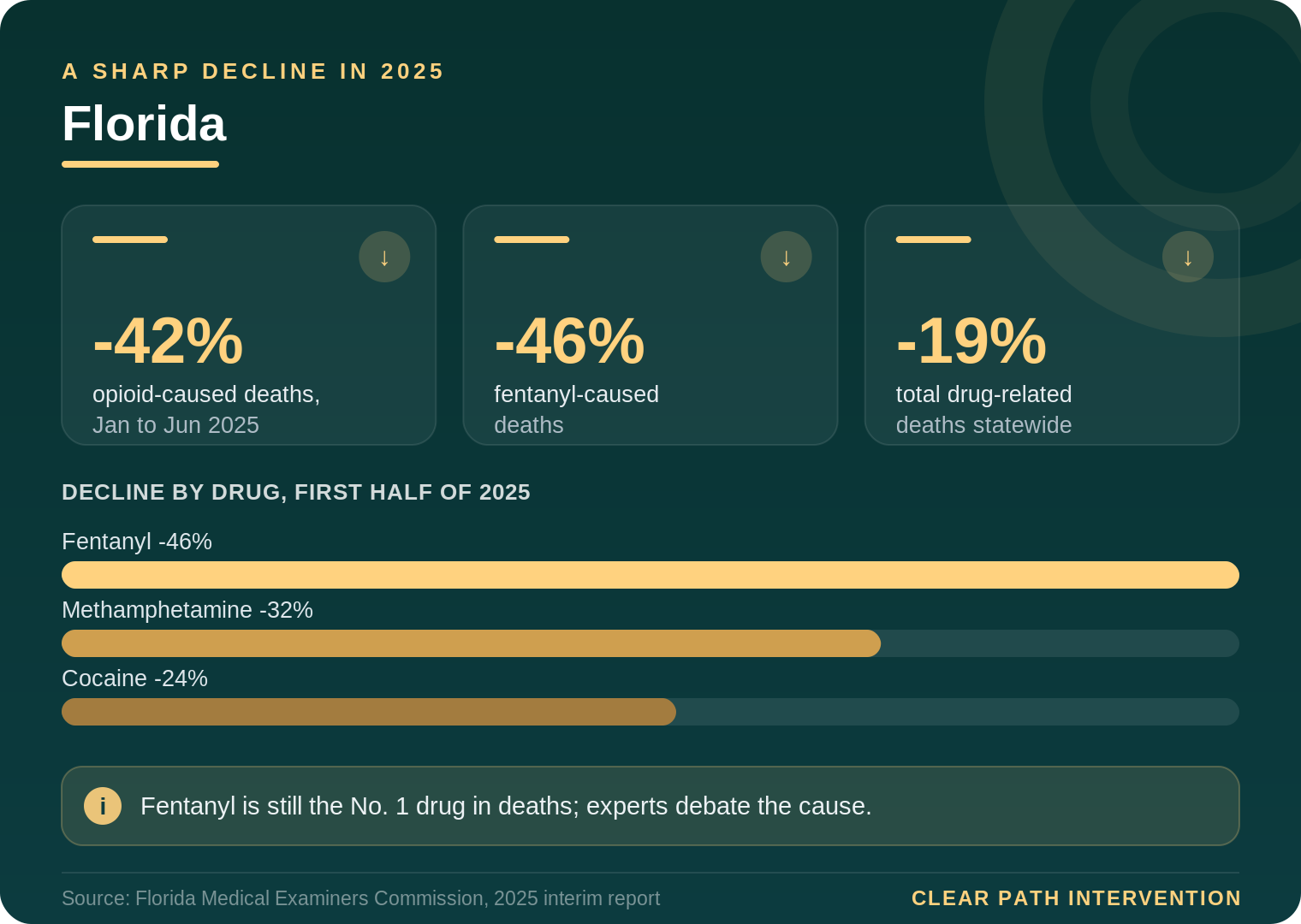
Start with the good news, because it is substantial. In May 2026, the Florida Department of Law Enforcement reported that, for the first half of 2025, opioid-caused deaths fell 42 percent and fentanyl-caused deaths fell 46 percent compared with the year before, with total drug-related deaths down 19 percent. As a company based in Pensacola, we have watched this trend take hold across our home state. It is real, and it is worth understanding clearly, including the parts that are still debated.
What is driving the decline, and what is contested
State leaders have credited stronger law enforcement and tougher trafficking penalties for the drop. But many researchers and harm-reduction specialists offer a more complicated explanation, and the disagreement is worth understanding rather than glossing over. As reported by Florida public radio, specialists point to shifts in the drug supply, wider availability of naloxone, and changes in patterns of use as major contributors, and note that the national decline has occurred across states with very different enforcement approaches. One University of Florida toxicologist observed that the sedative medetomidine has been swapping into the supply in place of xylazine, a change that alters the risk profile in ways enforcement statistics do not capture.
For families, the lesson in this debate is not which side is right. It is humility about easy explanations. The decline is real, but the danger has not been solved, and the same report that documented the drop confirmed that fentanyl remained the single leading drug in deaths, followed by cocaine and methamphetamine. A falling number is not the same as a safe environment. It is a reason for measured hope, not for looking away.
The history that still shapes Florida
To understand treatment in Florida, it helps to know two pieces of the state’s past, because both still echo. The first is the pill-mill era. In the late 2000s, Florida became the epicenter of prescription-opioid overprescribing, with pain clinics dispensing oxycodone at a scale that fed addiction across the entire eastern United States. The state eventually cracked down, but a generation of dependence had already taken root, and many of those people later moved to illicit opioids as the pills became harder to obtain.
The second is more delicate, and more important for families choosing help today. South Florida in particular became known for a troubling pattern in the addiction-treatment industry, sometimes called the Florida Shuffle, in which some operators profited by cycling vulnerable people through treatment programs and sober homes driven by insurance billing and referral money rather than genuine clinical care. Reputable providers across the state have spent years working to distinguish themselves from that history. But it is the reason a Florida family, more than almost anywhere else, should ask hard questions about how any treatment recommendation is being made, and whether the person making it has a financial stake in where their loved one is sent.
How the crisis looks across Florida
Florida is vast and varied, and the interventionists who work with families across Florida see distinct regional realities from the Panhandle to the Keys.
Miami and Fort Lauderdale
South Florida holds the densest concentration of the state’s treatment industry, which means families in the Miami and Fort Lauderdale areas have abundant options and the greatest need to vet them carefully. This is the region where the Florida Shuffle took root, and where clinical fit, rather than who pays a referral fee, should drive every placement decision.
Tampa Bay
The Tampa region sits along Gulf trafficking routes and has seen the same fentanyl-dominant, increasingly polysubstance pattern documented statewide, with cocaine and methamphetamine frequently present alongside opioids.
Orlando and Central Florida
A large and fast-growing metro built heavily on tourism and shift work, the Orlando area reflects the pressures of an economy with irregular hours and a transient population, conditions that can complicate both the onset of addiction and the path to steady treatment.
Pensacola and the Panhandle
In our home region, the Pensacola area and the broader Panhandle share more in common with the rural Deep South than with South Florida, including thinner treatment resources spread across longer distances. Families here often have to travel for specialized care, which makes preparation and coordination a central part of any plan.
How to vet a treatment program in Florida
Given the state’s history, knowing how to evaluate a treatment program is as important in Florida as the decision to seek one. The Florida Shuffle worked precisely because desperate families, in crisis, rarely had the time or knowledge to scrutinize where their loved one was being sent. A few questions, asked before committing, can separate reputable care from the operators who gave the industry its troubled reputation.
Ask how the program is licensed and accredited, and by whom. Legitimate facilities hold state licensure and often national accreditation, and they will answer the question directly. Ask what the clinical model is, and whether it includes medication for opioid use disorder where appropriate, since the strongest evidence supports medication-assisted treatment for opioids rather than abstinence-only approaches. Ask who owns the program and how it is paid, and whether anyone recommending it receives compensation for the referral. Ask what happens after the initial stay, because recovery depends heavily on continuing care, and reputable programs plan for it rather than discharging people into a vacuum.
Be cautious of certain signals. Aggressive marketing, promises of guaranteed success, offers to pay for travel or to waive costs in exchange for using insurance, and pressure to decide immediately are all patterns associated with the worst of the industry. A program that treats a family’s questions as reasonable, rather than as obstacles, is showing something important about how it operates.
This scrutiny is not cynicism. It is the appropriate response to a real history, and it protects the most important thing a family has: the narrow window in which a loved one is willing to accept help. Sending someone to the wrong program can squander that willingness and make the next attempt harder. The goal is to ensure that when a loved one finally says yes, the help waiting on the other side is genuine.
What the evidence says about getting someone into care
Given Florida’s particular history, the question of trust deserves to sit at the center of how a family approaches help. Some intervention providers and referral services accept compensation from the treatment centers they recommend, a practice that can quietly steer a loved one toward whoever pays rather than whoever fits. Families are entitled to ask anyone they work with whether that is the case, and to expect placements based on clinical need. In a state with Florida’s past, that question is not rude. It is responsible.
On the method itself, the approaches with the best evidence share a reliance on preparation rather than the dramatic confrontation television tends to depict. The Johnson Model gathers a prepared group to express concern and present a clear path to treatment. Family-systems methods such as ARISE, and the research-supported CRAFT approach (Community Reinforcement and Family Training), place more weight on coaching the family in communication and reinforcement, and CRAFT has been found in controlled studies to engage a substantial share of previously treatment-resistant people. The clinical guidance compiled by SAMHSA consistently finds that structured family involvement improves outcomes.
The science beneath all of this counters the moral framing families often slip into. Addiction alters the brain systems governing judgment, reward, and self-control, a process documented in NIDA’s research on drug misuse and addiction, which is part of why a loved one often cannot weigh their own risk accurately and why the people around them end up carrying some of that judgment. A useful plan also includes a treatment placement arranged in advance, so that a yes can be acted on the same day rather than lost to delay.
Florida’s decline is a hopeful chapter, and the people who worked to bring those numbers down deserve credit. But the state’s history is a reminder that progress and exploitation can coexist, and that a family’s job is not only to get a loved one to say yes, but to make sure the help on the other side of that yes is real. Understanding both the encouraging data and the complicated backdrop is what allows a family to navigate Florida’s landscape with clear eyes.
For continuing context, the CDC overdose prevention center tracks national and state data, and the Florida Medical Examiners Commission publishes its Drugs in Deceased Persons reports. Anyone in immediate crisis can reach the SAMHSA National Helpline at 1-800-662-HELP or dial 988.
HELP IS AVAILABLE
Do You Have a Loved One Struggling with Addiction or Mental Health Issues?

There is a particular kind of exhaustion that comes from loving someone whose drug addiction has taken over their life. You have had the conversations. You have made the threats — and not followed through. You have set boundaries — and let them slip. You have searched online at 2 a.m. and closed the laptop […]

When a family is in crisis — when a loved one’s addiction has reached the point where something has to happen — the pressure to act quickly can make it hard to think clearly about who to call. The intervention field is largely unregulated. Anyone can call themselves an interventionist. The quality of services ranges […]

Families who are new to this process often have a narrow picture of what a professional intervention service involves. A specialist shows up, talks to the family for a bit, sits in the room during the conversation, and leaves. That picture is missing most of what actually happens — and most of what makes the […]

Families who are new to the process of addressing a loved one’s addiction often use the words “intervention” and “treatment” interchangeably. It is an understandable confusion. Both are part of the path toward recovery. Both involve professionals. But they are not the same thing, and confusing them can delay getting the right kind of help […]