by Clear Path Intervention
Share
by Clear Path Intervention
Share
")
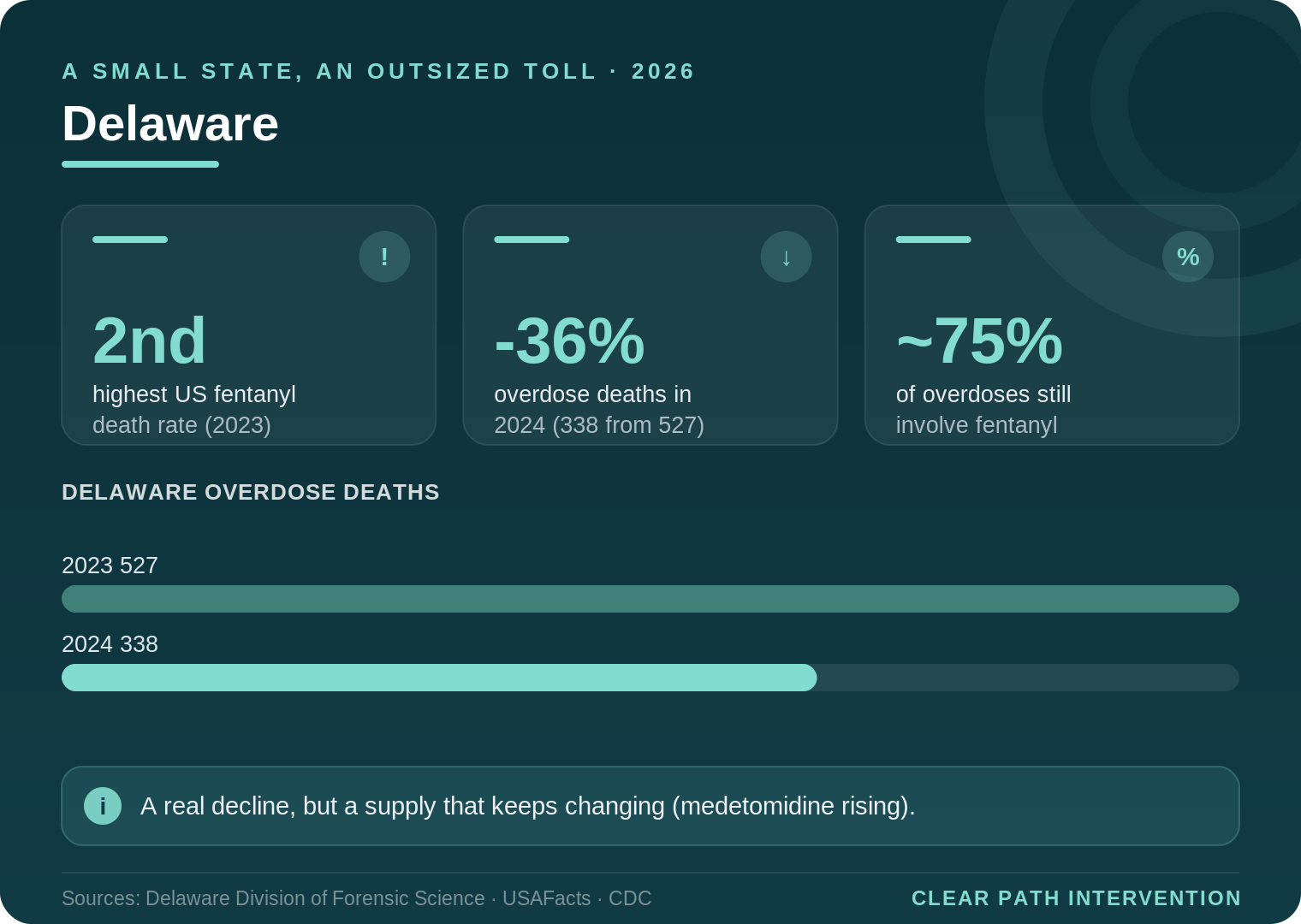
Delaware is one of the smallest states in the country, and for years it carried one of the heaviest overdose burdens, measured against its size. By the most recent national comparisons, Delaware ranked second only to West Virginia in its rate of fentanyl-involved overdose deaths. A small population, an outsized loss. That history is what makes the state’s recent turn so striking, and worth examining carefully.
Because in 2024, the numbers fell hard. According to state agency data reported by Delaware Public Media, the state recorded 338 confirmed overdose deaths in 2024, down about 36 percent from 527 in 2023. For a state that had watched the toll climb year after year, a decline of that size is a genuine turning point. The question every family should sit with is what it means, and how durable it is.
Reading the decline honestly
A 36 percent drop is the kind of number that invites celebration, and there is reason for some. The decline tracks a broader regional and national improvement that researchers attribute to several factors working together: far wider distribution of the overdose-reversal medication naloxone, expanded access to medication for opioid use disorder, harm-reduction tools such as fentanyl test strips, and possibly a shift in the illicit supply itself. Delaware invested in these approaches, including harm-reduction vending machines and broader Narcan access, and the timing lines up with the regional trend.
At the same time, state officials have been careful not to declare victory, and families should adopt the same caution. Fentanyl still drives roughly three quarters of the state’s overdoses. And the supply is not standing still. Delaware saw xylazine ease somewhat in late 2024, only to see a rise in medetomidine, another veterinary sedative unsafe for humans that can cause serious respiratory and cardiac effects and, notably, a withdrawal that can be life-threatening on its own. Cocaine continues to appear in a growing share of deaths. A lower death count does not mean a safer supply. It means the rescue and treatment systems are catching more people, for now.
Why geography concentrates the problem
Part of Delaware’s outsized burden has always been about position. The state sits on the Interstate 95 corridor between Baltimore and Philadelphia, one of the most heavily trafficked drug routes on the East Coast. Supply moving along that corridor has historically kept Delaware’s availability high relative to its size, which is one reason a small state ended up with a death rate among the nation’s worst. Geography does not cause addiction, but it shapes how much of a dangerous supply reaches a given community, and Delaware has long been exposed.
For families, that exposure is the backdrop against which an individual’s struggle plays out. It means the drugs are close, cheap, and contaminated, and that the gap between a developing problem and a fatal outcome can be short. The recent decline does not change that underlying geography. It only means the state has gotten somewhat better at intervening before the worst happens.
How the crisis looks across Delaware
The interventionists who work with families across Delaware encounter the state’s three counties as distinct environments, even within so compact a geography.
Wilmington and New Castle County
The state’s largest population center, anchored by Wilmington, has consistently carried the heaviest share of Delaware’s overdose deaths, and its position near the I-95 corridor keeps the supply close. It also holds the deepest concentration of treatment resources in the state, which gives families here a relative advantage in reaching care quickly.
Dover and Kent County
The capital region occupies a middle ground, with a mix of urban and rural communities and treatment resources that thin as one moves away from the city. Families in central Delaware often face longer distances to specialized care than those in the north.
Sussex County and the southern shore
Delaware’s southern county is its most rural, and the access challenges that define rural addiction nationally apply here too. The distance to appropriate treatment can be a real factor in planning, which makes preparation and logistics part of any effective response rather than an afterthought.
Recognizing the warning signs, and the small-state factor
For families wondering whether what they are seeing warrants action, the honest answer is that waiting for certainty usually means waiting too long. Addiction rarely announces itself in a single dramatic moment. More often it is a slow accumulation of changes that, taken together, tell the story: withdrawal from family and longtime friends, a new and secretive social circle, money that goes missing, declining performance at work or school, and a defensiveness that surfaces around ordinary questions. Physical signs such as changes in sleep, weight, or appearance tend to come later, which is why families who wait for visible deterioration often act late.
Delaware’s size adds a particular wrinkle. In a small state where communities are tightly knit and word travels, families sometimes feel a heightened pressure to keep a loved one’s struggle private. That instinct is understandable, but secrecy tends to delay care, and delay is precisely what the current supply punishes most severely. Treating addiction as the medical condition it is, rather than a private shame to be managed quietly, is frequently the first practical step toward getting help.
It also helps to understand why a struggling person so rarely raises the issue themselves. The same brain changes that drive continued use impair insight into the problem. This is not stubbornness in the ordinary sense. It is a genuine difficulty perceiving the situation accurately, which is why the people around a person often recognize the danger before the person does. In a state where the supply has been among the deadliest in the nation, that outside perspective is not interference. It can be lifesaving.
The emergence of medetomidine reinforces the point. Because its withdrawal can be hazardous, medically supervised detoxification matters, and a loved one’s attempt to simply stop on their own may be both unlikely to succeed and medically risky. None of this requires a family to be certain or to have a complete plan before reaching out. Most families who seek help know only that something is wrong and that their own efforts have stopped working. In a state that has lost so many, that recognition is reason enough to act.
What the evidence says about getting someone into care
The fragility of Delaware’s progress is itself an argument for acting rather than waiting. A statewide decline says nothing about whether a particular person is safer, especially when the supply that remains is still dominated by fentanyl and is absorbing new and unpredictable adulterants. The lever that changes an individual’s odds is the same one that moved the state’s numbers: getting the person into treatment.
When families decide to act, the credible approaches share an emphasis on preparation over confrontation. The Johnson Model assembles a prepared group to express concern and offer a clear route to care. Family-systems methods such as ARISE, and the research-supported CRAFT approach, place greater weight on coaching the family in communication and positive reinforcement, and CRAFT in particular has been found in controlled studies to engage a meaningful share of previously resistant people. The clinical guidance compiled by SAMHSA consistently points toward structured family involvement as a factor that improves outcomes.
It also helps to understand why a loved one rarely initiates this on their own. Addiction alters the brain circuits governing judgment and self-control, a process detailed in NIDA’s research on drug misuse and addiction, which leaves many people genuinely unable to weigh their own risk accurately. The emergence of medetomidine adds a clinical wrinkle worth knowing: because its withdrawal can be dangerous, medically supervised detoxification matters more than ever, and attempting to quit cold turkey without support can be hazardous. This is one more reason a professional assessment of what a person is actually using is a sensible first step.
Delaware’s turning point is real, and it deserves to be recognized as the product of deliberate public health work rather than luck. But a turning point is not a destination. For a small state that has lost so many, the recent decline is best understood as evidence that the tools work, and as a reason to use them, quickly, for the people still at risk. The numbers came down because people reached care. The same path is open to any family willing to take it.
Delaware’s progress shows what is possible when a community commits to keeping people alive and connecting them to care. For any family still in the middle of it, that same possibility is within reach, and the most useful step is rarely to wait. It is to seek informed guidance while the window is open, and to treat a loved one’s struggle as the medical emergency it can quietly become.
For continuing context, the CDC overdose prevention center and KFF both track state and national overdose data. Anyone in immediate crisis can reach the SAMHSA National Helpline at 1-800-662-HELP or dial 988.
HELP IS AVAILABLE
Do You Have a Loved One Struggling with Addiction or Mental Health Issues?

For most of the country, 2025 brought the first real relief from the fentanyl crisis in years. Colorado got a different report. While national overdose deaths fell sharply, Colorado became one of a small group of states where the numbers turned back upward, and its largest city recorded one of its worst years on record. […]

California does not fit the story most people carry in their heads about the overdose crisis. It is, by prescribing measures, one of the most cautious states in the country. It also contains some of the most visible, concentrated drug crises in America. Both things are true at once, and holding them together is the […]

Every state’s addiction story has a starting point. In Arkansas, more than in almost anywhere else in the country, that story began at the pharmacy counter. For years the state has led or nearly led the nation in how many opioid prescriptions its doctors write, and that history still shapes the crisis families face today. […]

The national story about overdose in 2026 is, for once, a hopeful one. Deaths have fallen for several years running. Arizona is the exception to that story. While the rest of the country has been recording its first sustained relief from the fentanyl crisis, Arizona has been moving in the opposite direction, and the gap […]