by Clear Path Intervention
Share
by Clear Path Intervention
Share

For most of the country, 2025 brought the first real relief from the fentanyl crisis in years. Colorado got a different report. While national overdose deaths fell sharply, Colorado became one of a small group of states where the numbers turned back upward, and its largest city recorded one of its worst years on record. For families here, that divergence is not an abstraction. It means the broad reassurance other Americans are reading does not describe their state, and the danger surrounding a struggling loved one has grown rather than eased.
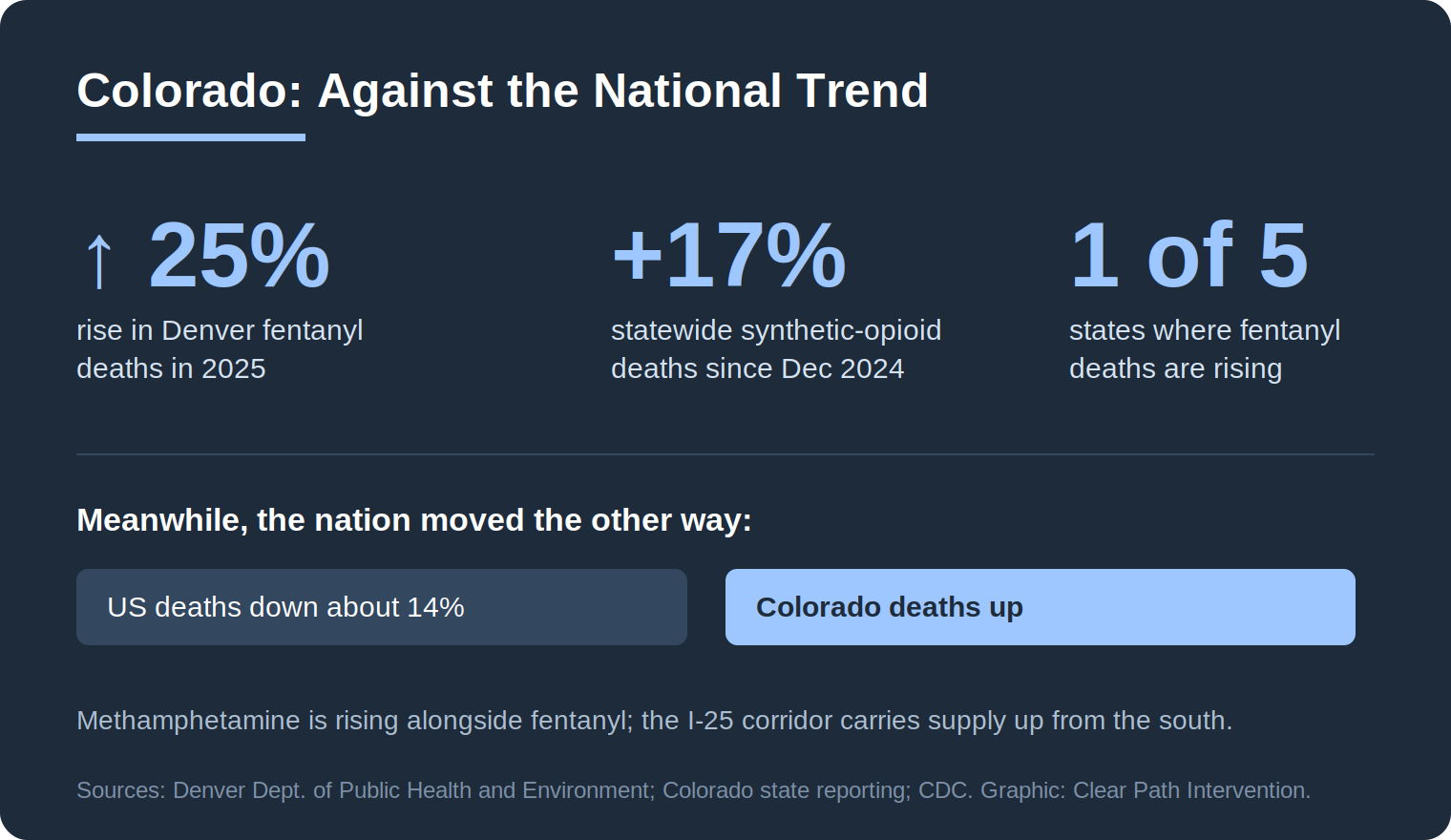
The clearest signal came from Denver. In January 2026, the city’s health department reported that fatal fentanyl overdoses rose nearly 25 percent in 2025, putting Denver on track for a record year with more than 400 overdose deaths projected. Methamphetamine deaths rose in the city as well. This was happening while the national death count was dropping by double digits.
A second spike, not a continuation
What makes Colorado’s situation distinct is its shape. This is not a crisis that simply never improved. Colorado, like the rest of the country, saw fentanyl deaths peak in late 2023 and then ease through 2024. The problem is what came next. Beginning in late 2024 and running through 2025, the numbers climbed again. Analysts describe synthetic-opioid overdose deaths in Colorado growing by roughly 17 percent since December 2024, among the fastest increases in the nation, even as the national rate fell over the same window. Reporting has identified Colorado as one of only about five states, alongside Arizona, New Mexico, Montana, and South Dakota, where fentanyl deaths have been rising rather than falling.
This second-spike pattern is part of why the broad national story can be misleading at the state level. Researchers have linked the national decline partly to a disruption in the illicit fentanyl supply, possibly tied to actions by the Chinese government affecting precursor chemicals. But supply disruptions are uneven. In places where the supply has stayed cheap and plentiful, the improvement did not arrive, or arrived and then reversed. Colorado appears to be one of those places.
Why Denver became a hotspot
Geography is a large part of the explanation. Denver sits along the Interstate 25 corridor, a direct route that traffickers use to move fentanyl and methamphetamine north from the southern border into the Rocky Mountain region. Federal seizure data has shown sharp increases in the volume of fentanyl pills intercepted in Colorado, an indicator that local availability has not eased the way it has elsewhere. When the supply remains abundant, the exposure remains constant, and the death toll follows.
Two further details from Denver’s data are worth noting for families. First, methamphetamine deaths rose alongside fentanyl, reinforcing that this is a polysubstance crisis rather than a single-drug one. Second, overdoses remain the leading cause of death for people experiencing homelessness in the city, a reminder that the crisis falls hardest on the most vulnerable and least connected to care. The throughline is access. People die when they cannot reach treatment, and the supply does not wait.
The policy backdrop, briefly
Colorado’s recent history also illustrates how hard this problem is to legislate. The state moved in 2019 to reduce penalties for low-level drug possession, then reversed course in 2022 as fentanyl deaths mounted, making possession of larger quantities a felony. The 2022 law, however, applied only when a person was knowingly carrying fentanyl, a difficult thing to prove given how often fentanyl is mixed invisibly into other drugs. The point for families is not which policy was correct. It is that enforcement and legislation, whatever their merits, have not by themselves protected individuals. The thing that reliably changes a person’s odds is getting them into treatment.
How the crisis looks across Colorado
The interventionists who work with families across Colorado encounter different versions of the problem depending on the community.
Denver
As the epicenter of the state’s resurgence, the Denver metro carries both the heaviest overdose burden and the deepest concentration of treatment resources. The advantage of proximity is real here, but so is the intensity of an abundant supply. Acting before a crisis forces the issue is the part a family can control.
Colorado Springs
Home to a large military and veteran population, the Colorado Springs area sees the particular intersection of addiction with service-related trauma and chronic pain. Co-occurring conditions, where a substance problem sits alongside post-traumatic stress or depression, are common, and they make professional assessment especially valuable.
Aurora
Colorado’s third-largest city, the Aurora area shares much of the metro Denver supply picture, with a diverse, growing population and the same polysubstance pressures seen across the Front Range.
Fort Collins and the northern Front Range
Anchored by Colorado State University, the Fort Collins region, along with nearby Boulder, contends with the young-adult patterns common to college towns: experimentation that meets a contaminated supply, where a single counterfeit pill can carry a fatal dose. The danger for this age group is less chronic addiction than the lethality of a first or occasional exposure.
Practical protection while the supply stays dangerous
While the larger work of getting a loved one into treatment proceeds, there are concrete steps that reduce the immediate risk of death, and families in a high-supply environment like Colorado’s have reason to know them. The overdose-reversal medication naloxone is available without a prescription in Colorado, including free through many public health programs, and it has reversed thousands of overdoses statewide. Fentanyl test strips, also distributed through harm-reduction programs, let a person check whether a substance contains fentanyl, which matters enormously given how often it is mixed invisibly into other drugs.
Some families hesitate at these measures, worried that acknowledging the risk amounts to condoning use. The evidence points the other way. Keeping a person alive is the precondition for everything else, and naloxone in a parent’s bag or a partner’s glove compartment has bought countless families the time to get a loved one into care. Harm reduction and recovery are not opposing philosophies. One keeps a person alive long enough for the other to work. None of this replaces treatment, but in a state where the supply is growing more lethal, it is a reasonable layer of protection while the larger plan comes together.
What a rising trend changes, and what it does not
It is important to be careful about what Colorado’s numbers mean. A rising statewide death count does not make recovery less possible. Treatment works the same way in Denver as it does in cities where the trend is falling. What changes is the risk environment around a person who has not yet entered care. In a state where the supply is growing more lethal rather than less, the cost of waiting is higher, and the familiar instinct to hold out for rock bottom is more dangerous than usual.
That instinct deserves direct examination, because the research complicates it. Motivation and readiness frequently follow entry into treatment rather than preceding it, which is part of why early, structured family action is associated with better outcomes than passive waiting. The science underneath this is consistent: addiction alters the brain systems governing judgment and self-control, as documented in NIDA’s research on drug misuse and addiction, which means a loved one often cannot accurately assess their own escalating risk. Someone has to do part of that assessing for them.
When a family decides to act, the credible approaches share a reliance on preparation rather than surprise. Structured methods such as the research-supported CRAFT model, documented in clinical guidance gathered by SAMHSA, coach families in communication and reinforcement and engage a substantial share of previously resistant people. Given the polysubstance reality in Colorado, an honest assessment of what a person is actually using is a sensible first step, and arranging a treatment placement in advance keeps a yes from slipping away.
The hopeful reading of Colorado’s hard numbers is the same one the national decline offers: the tools exist, and they save lives when people reach them. The state’s resurgence is a supply problem layered over those tools, not proof that the tools fail. For a family, the rising trend is a description of the environment, not a prediction about their loved one. Recovery remains possible. What 2026 adds is a reason not to wait.
Families do not need to navigate this alone, and they do not need every answer before they begin. Most arrive at the question of help knowing only that the situation has grown frightening and that their own attempts have not worked. In a state where the supply is moving the wrong way, that recognition is reason enough to seek informed guidance sooner rather than later.
For continuing context, the CDC overdose prevention center tracks national and state data, and the Colorado Department of Public Health and Environment publishes state overdose reporting. Anyone in immediate crisis can reach the SAMHSA National Helpline at 1-800-662-HELP or dial 988.
HELP IS AVAILABLE
Do You Have a Loved One Struggling with Addiction or Mental Health Issues?

There is a particular kind of exhaustion that comes from loving someone whose drug addiction has taken over their life. You have had the conversations. You have made the threats — and not followed through. You have set boundaries — and let them slip. You have searched online at 2 a.m. and closed the laptop […]

When a family is in crisis — when a loved one’s addiction has reached the point where something has to happen — the pressure to act quickly can make it hard to think clearly about who to call. The intervention field is largely unregulated. Anyone can call themselves an interventionist. The quality of services ranges […]

Families who are new to this process often have a narrow picture of what a professional intervention service involves. A specialist shows up, talks to the family for a bit, sits in the room during the conversation, and leaves. That picture is missing most of what actually happens — and most of what makes the […]

Families who are new to the process of addressing a loved one’s addiction often use the words “intervention” and “treatment” interchangeably. It is an understandable confusion. Both are part of the path toward recovery. Both involve professionals. But they are not the same thing, and confusing them can delay getting the right kind of help […]